

doi: 10.1155/2013/401359.
Epub 2013 Apr 29.
Combined awake craniotomy with endoscopic port surgery for resection of a deep-seated temporal lobe glioma: a case report
Affiliations
- PMID: 23737799
- PMCID: PMC3657435
- DOI: 10.1155/2013/401359
Item in Clipboard
Combined awake craniotomy with endoscopic port surgery for resection of a deep-seated temporal lobe glioma: a case report
Case Rep Med.
2013.
Abstract
The authors describe the combination of awake craniotomy and minimally invasive endoscopic port surgery to resect a high-grade glioma located near eloquent structures of the temporal lobe. Combined minimally invasive techniques such as these may facilitate deep tumor resection within eloquent regions of the brain, allowing minimum white matter dissection. Technical aspects of this procedure, a case outcome involving this technique, and the direction of further investigations for the utility of these techniques are discussed.
Figures
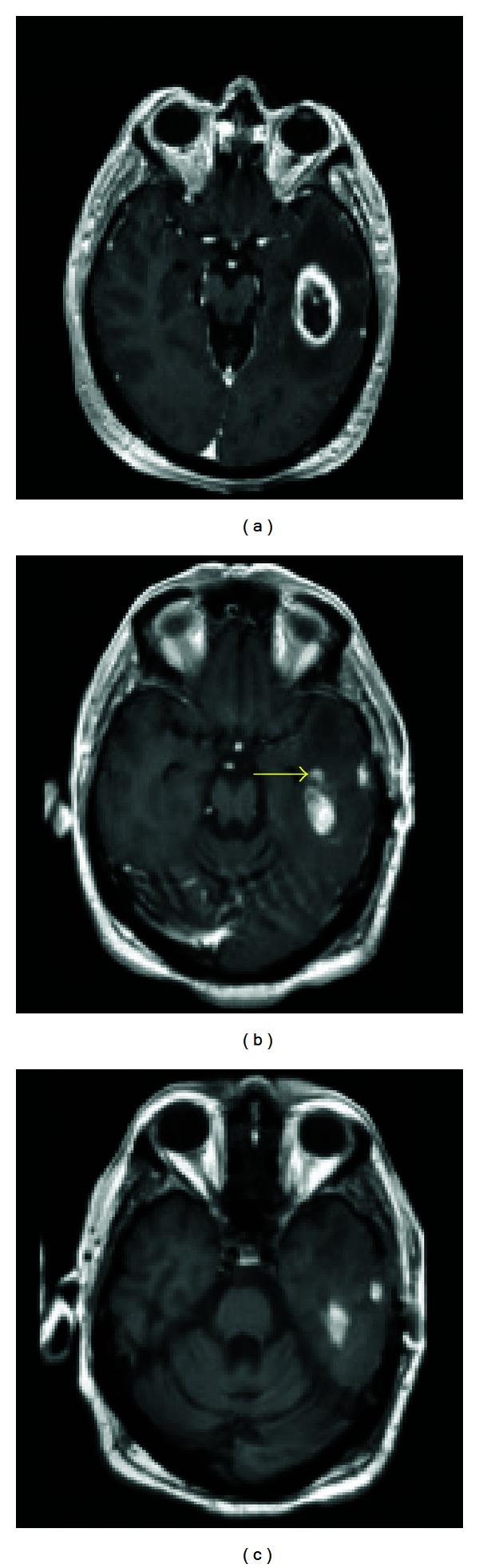
Preoperative and postoperative images. (a) Preresection T1 axial MRI with contrast showing a temporal lesion with an estimated 5.0 cubic centimeter volume. (b) Immediate postresection T1 axial MRI with contrast showing a slight amount of residual enhancement at the anteromedial margin of the resection cavity. (Yellow arrow indicates residual tumor area not present in (c)). (c) The corresponding noncontrast enhanced T1 MRI image taken at the same time demonstrates that the posteromedial and lateral hyperintensities are in fact blood products and postoperative change rather than gross residual tumor. A 93.3% volumetric resection was achieved.
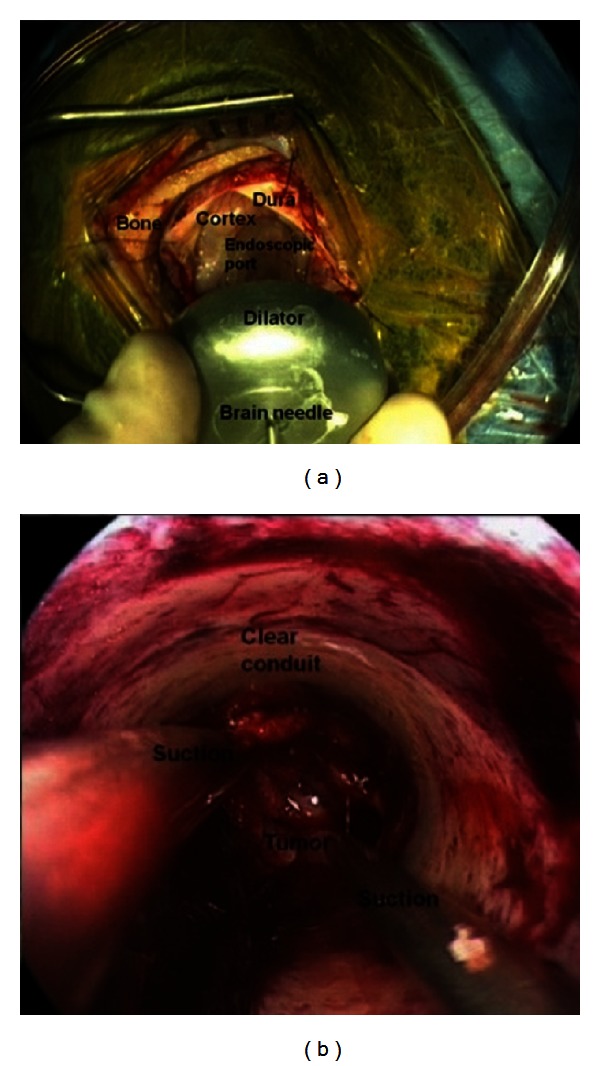
(a) View of the endoscopic port with dilator insertion and (b) surgical view through the endoscopic port.
References
-
- July J, Manninen P, Lai J, Yao Z, Bernstein M. The history of awake craniotomy for brain tumor and its spread into Asia. Surgical Neurology. 2009;71(5):621–624. - PubMed
-
- Haglund MM, Berger MS, Shamseldin M, et al. Cortical localization of temporal lobe language sites in patients with gliomas. Neurosurgery. 1994;34(4):567–576. - PubMed
-
- Shinoura N, Yamada R, Tabei Y, Saito K, Suzuki Y, Yagi K. Advantages and disadvantages of awake surgery for brain tumours in the primary motor cortex: institutional experience and review of literature. British Journal of Neurosurgery. 2011;25(2):218–224. - PubMed
-
- Szelényi A, Bello L, Duffau H, et al. Intraoperative electrical stimulation in awake craniotomy: methodological aspects of current practice. Neurosurgical Focus. 2010;28(2):E7.1–E7.8. - PubMed
-
- Abernathey CD, Davis DH, Kelly PJ. Treatment of colloid cysts of the third ventricle by stereotaxic microsurgical laser craniotomy. Journal of Neurosurgery. 1989;70(4):525–529. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
