

Minimally invasive direct repair of bilateral lumbar spine pars defects in athletes
- PMID: 23737800
- PMCID: PMC3657441
- DOI: 10.1155/2013/659078
Minimally invasive direct repair of bilateral lumbar spine pars defects in athletes
Abstract
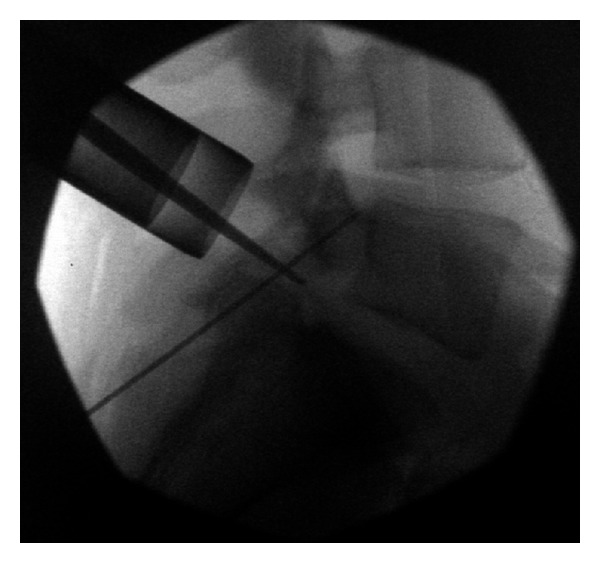
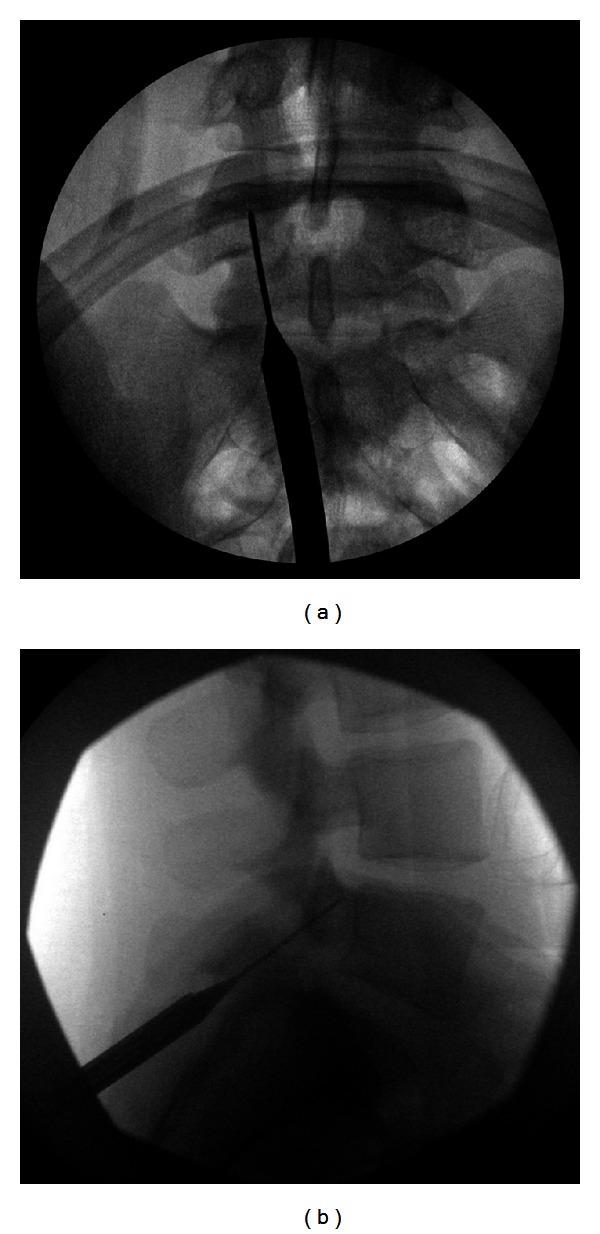
Spondylolysis of the lumbar spine has traditionally been treated using a variety of techniques ranging from conservative care to fusion. Direct repair of the defect may be utilized in young adult patients without significant disc degeneration and lumbar instability. We used minimally invasive techniques to place pars interarticularis screws with the use of an intraoperative CT scanner in three young adults, including two athletes. This technique is a modification of the original procedure in 1970 by Buck, and it offers the advantage of minimal muscle dissection and optimal screw trajectory. There were no intra- or postoperative complications. The detailed operative procedure and the postoperative course along with a brief review of pars interarticularis defect treatment are discussed.
Figures




References
-
- Bell DF, Ehrlich MG, Zaleske DJ. Brace treatment for symptomatic spondylolisthesis. Clinical Orthopaedics and Related Research. 1988;(236):192–198. - PubMed
-
- Higashino K, Sairyo K, Katoh S, Sakai T, Kosaka H, Yasui N. Minimally invasive technique for direct repair of the pars defects in young adults using a spinal endoscope: a technical note. Minimally Invasive Neurosurgery. 2007;50(3):182–186. - PubMed
-
- Brennan RP, Smucker PY, Horn EM. Minimally invasive image-guided direct repair of bilateral L-5 pars interarticularis defects: technical note. Neurosurgical Focus. 2008;25(2, article E13) - PubMed
-
- Lim MR, Yoon SC, Green DW. Symptomatic spondylolysis: diagnosis and treatment. Current Opinion in Pediatrics. 2004;16(1):37–46. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
