

If you don't find it often, you often don't find it: why some cancers are missed in breast cancer screening
- PMID: 23737980
- PMCID: PMC3667799
- DOI: 10.1371/journal.pone.0064366
If you don't find it often, you often don't find it: why some cancers are missed in breast cancer screening
Abstract
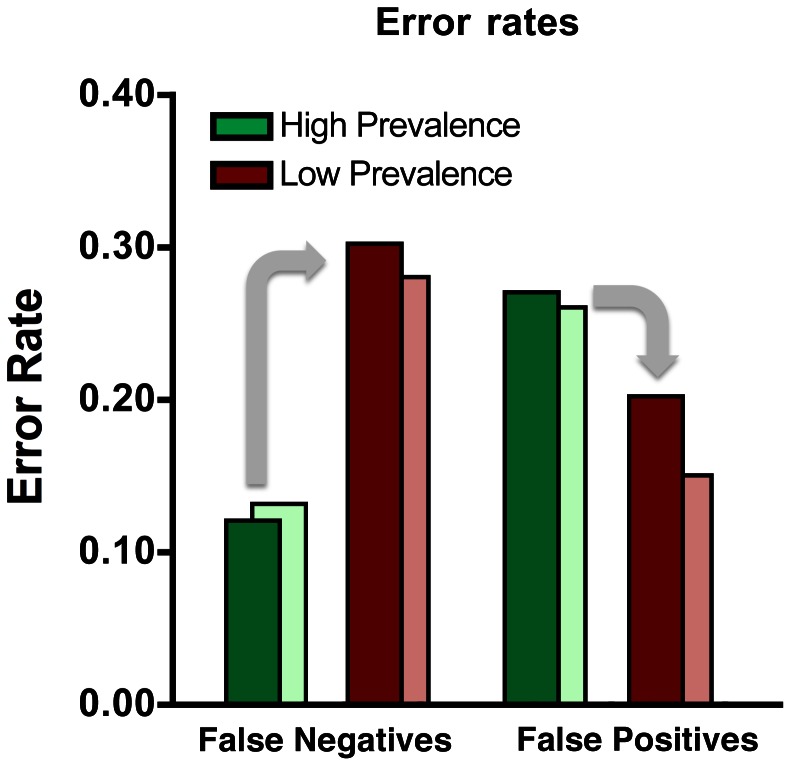
Mammography is an important tool in the early detection of breast cancer. However, the perceptual task is difficult and a significant proportion of cancers are missed. Visual search experiments show that miss (false negative) errors are elevated when targets are rare (low prevalence) but it is unknown if low prevalence is a significant factor under real world, clinical conditions. Here we show that expert mammographers in a real, low-prevalence, clinical setting, miss a much higher percentage of cancers than are missed when the mammographers search for the same cancers under high prevalence conditions. We inserted 50 positive and 50 negative cases into the normal workflow of the breast cancer screening service of an urban hospital over the course of nine months. This rate was slow enough not to markedly raise disease prevalence in the radiologists' daily practice. Six radiologists subsequently reviewed all 100 cases in a session where the prevalence of disease was 50%. In the clinical setting, participants missed 30% of the cancers. In the high prevalence setting, participants missed just 12% of the same cancers. Under most circumstances, this low prevalence effect is probably adaptive. It is usually wise to be conservative about reporting events with very low base rates (Was that a flying saucer? Probably not.). However, while this response to low prevalence appears to be strongly engrained in human visual search mechanisms, it may not be as adaptive in socially important, low prevalence tasks like medical screening. While the results of any one study must be interpreted cautiously, these data are consistent with the conclusion that this behavioral response to low prevalence could be a substantial contributor to miss errors in breast cancer screening.
Conflict of interest statement
Figures
References
-
- Kopans DB, Smith RA, Duffy SW (2011) Mammographic screening and "overdiagnosis". Radiology 260(3): 616–20. - PubMed
-
- Berlin L (2007) Accuracy of diagnostic procedures: has it improved over the past five decades? American Journal of Roentgenology 188(5): 1173–8. - PubMed
-
- Bird RE, Wallace TW, Yankaskas BC (1992) Analysis of cancers missed at screening mammography. Radiology 184(3): 613. - PubMed
-
- Majid AS, de Paredes ES, Doherty RD, Sharma NR, Salvador X (2003) Missed breast carcinoma: pitfalls and pearls. Radiographics 23(4): 881. - PubMed
-
- Boyer B, Hauret L, Bellaiche R, Graf C, Bourcier B, et al. (2004) Retrospectively detectable carcinomas: review of the literature. Journal de Radiologie 85: 2071–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
