

Parasitic infection may be associated with discordant responses to QuantiFERON and tuberculin skin test in apparently healthy children and adolescents in a tuberculosis endemic setting, Ethiopia
- PMID: 23738853
- PMCID: PMC3674899
- DOI: 10.1186/1471-2334-13-265
Parasitic infection may be associated with discordant responses to QuantiFERON and tuberculin skin test in apparently healthy children and adolescents in a tuberculosis endemic setting, Ethiopia
Abstract
Background: M. tuberculosis remains one of the world's deadliest pathogens in part because of its ability to establish persistent, latent infections, which can later reactivate to cause disease. In regions of the globe where disease is endemic, as much as 50% of the population is thought to be latently infected, complicating diagnosis and tuberculosis control. The tools most commonly used for diagnosis of latent M. tuberculosis infection are the tuberculin skin test and the newer interferon-gamma release assays, both of which rely on an antigen-specific memory response as an indicator of infection. It is clear that the two tests, do not always give concordant results, but the factors leading to this are only partially understood.
Methods: In this study we examined 245 healthy school children aged from 12 to 20 years from Addis Ababa, a tuberculosis-endemic region, characterised them with regard to response in the tuberculin skin test and QuantIFERON™ test and assessed factors that might contribute to discordant responses.
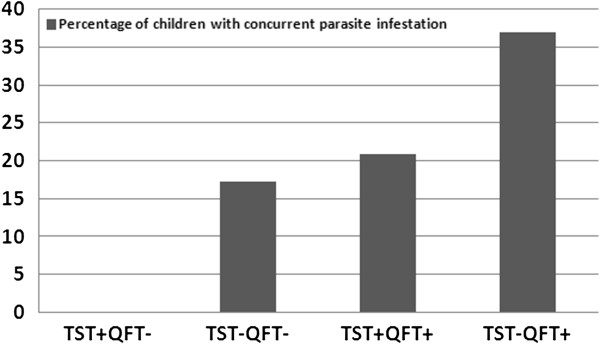
Results: Although concordance between the tests was generally fair (90% concordance), there was a subset of children who had a positive QuantIFERON™ result but a negative tuberculin skin test. After analysis of multiple parameters the data suggest that discordance was most strongly associated with the presence of parasites in the stool.
Conclusions: Parasitic gut infections are frequent in most regions where M. tuberculosis is endemic. This study, while preliminary, suggests that the tuberculin skin test should be interpreted with caution where this may be the case.
Figures
References
-
- World Health Organization. Global Tuberculosis Control. Epidemiology, Strategy, Financing. Geneva: WHO; 2009.
-
- Kabra SK, Lodha R, Seth V. Some current concepts on childhood tuberculosis. Indian J Med Res. 2004;120(4):387–397. - PubMed
-
- Federal Ministry of Health. Tuberculosis, Leprosy and TB/HIV Prevention and Control Programme: Manual. 4. Ethiopia; 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
