

Long term effect of depression care management on mortality in older adults: follow-up of cluster randomized clinical trial in primary care
- PMID: 23738992
- PMCID: PMC3673762
- DOI: 10.1136/bmj.f2570
Long term effect of depression care management on mortality in older adults: follow-up of cluster randomized clinical trial in primary care
Abstract
Objective: To investigate whether an intervention to improve treatment of depression in older adults in primary care modified the increased risk of death associated with depression.
Design: Long term follow-up of multi-site practice randomized controlled trial (PROSPECT-Prevention of Suicide in Primary Care Elderly: Collaborative Trial).
Setting: 20 primary care practices in New York City, Philadelphia, and Pittsburgh, USA, randomized to intervention or usual care.
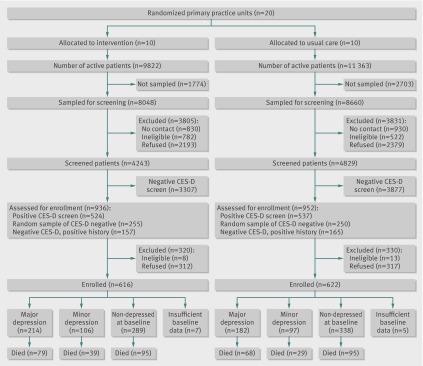
Participants: 1226 participants identified between May 1999 and August 2001 through a two stage, age stratified (60-74; ≥ 75 years) depression screening of randomly sampled patients; enrollment included patients who screened positive and a random sample of patients who screened negative.
Intervention: For two years, a depression care manager worked with primary care physicians in intervention practices to provide algorithm based care for depression, offering psychotherapy, increasing antidepressant dose if indicated, and monitoring symptoms, adverse effects of drugs, and adherence to treatment. This paper reports the long term follow-up.
Main outcome measure: Mortality risk based on a median follow-up of 98 (range 0.8-116.4) months through 2008.
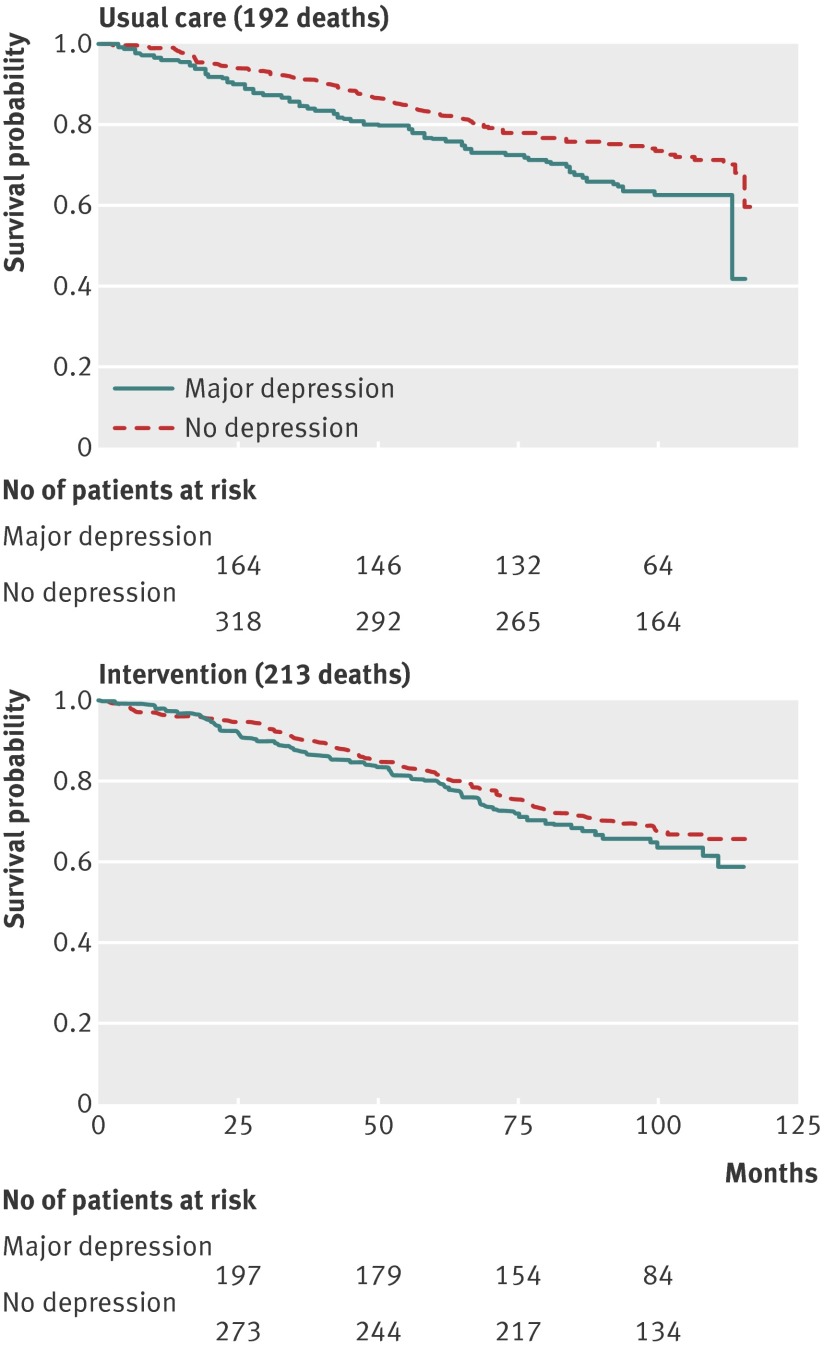
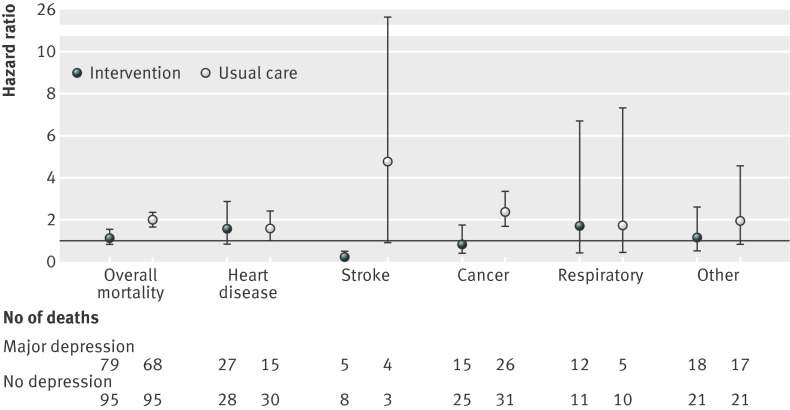
Results: In baseline clinical interviews, 396 people were classified as having major depression, 203 had clinically significant minor depression, and 627 did not meet criteria for depression. At follow-up, 405 patients had died. Patients with major depression in usual care were more likely to die than were those without depression (hazard ratio 1.90, 95% confidence interval 1.57 to 2.31). In contrast, patients with major depression in intervention practices were at no greater risk than were people without depression (hazard ratio 1.09, 0.83 to 1.44). Patients with major depression in intervention practices, relative to usual care, were 24% less likely to have died (hazard ratio 0.76, 0.57 to 1.00; P=0.05). Preliminary data on cause of death are provided. No significant effect on mortality was found for minor depression.
Conclusions: Older adults with major depression in practices provided with additional resources to intensively manage depression had a mortality risk lower than that observed in usual care and similar to older adults without depression.
Trial registration: Clinical trials NCT00000367.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Does treatment of depression in ageing populations decrease risk of mortality?Evid Based Med. 2014 Apr;19(2):60. doi: 10.1136/eb-2013-101470. Epub 2013 Sep 19. Evid Based Med. 2014. PMID: 24052396 No abstract available.
References
-
- Cuijpers P, Smit F. Excess mortality in depression: a meta-analysis of community studies. J Affect Disord 2002;72:227-36. - PubMed
-
- Schulz R, Drayer RA, Rollman BL. Depression as a risk factor for non-suicide mortality in the elderly. Biol Psychiatry 2002;52:205-25. - PubMed
-
- Mezuk B, Gallo JJ. Depression and medical illness in late life: race, resources, and stress. In: Lavretsky H, Sajatovic M, Reynolds CF, eds. Depression in late life. Oxford University Press, 2013:270-94.
-
- Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR, et al. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry 2005;58:175-89. - PubMed
-
- Ciechanowski PS, Katon WJ, Russo JE. Depression and diabetes: impact of depressive symptoms on adherence, function, and costs. Arch Intern Med 2000;160:3278-85. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R01 MH59366/MH/NIMH NIH HHS/United States
- P30 MH68638/MH/NIMH NIH HHS/United States
- P30 MH52129/MH/NIMH NIH HHS/United States
- R01 MH59381/MH/NIMH NIH HHS/United States
- K24 MH070407/MH/NIMH NIH HHS/United States
- P30 MH52247/MH/NIMH NIH HHS/United States
- K23 MH67671/MH/NIMH NIH HHS/United States
- T32 MH065218/MH/NIMH NIH HHS/United States
- K01MH073903/MH/NIMH NIH HHS/United States
- P30 MH085943/MH/NIMH NIH HHS/United States
- R01 MH59380/MH/NIMH NIH HHS/United States
- R01 MH065539/MH/NIMH NIH HHS/United States
- P30 MH090333/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical