

Management and outcomes of bowel obstruction in patients with stage IV colon cancer: a population-based cohort study
- PMID: 23739189
- PMCID: PMC4507563
- DOI: 10.1097/DCR.0b013e318294ed6b
Management and outcomes of bowel obstruction in patients with stage IV colon cancer: a population-based cohort study
Abstract
Background: Bowel obstruction is a common complication of late-stage abdominal cancer, especially colon cancer, which has been investigated predominantly in small, single-institution studies.
Objective: We used a large, population-based data set to explore the surgical treatment of bowel obstruction and its outcomes after hospitalization for obstruction among patients with stage IV colon cancer.
Design: This was a retrospective cohort study.
Setting and patients: We identified 1004 patients aged 65 years or older in the Surveillance, Epidemiology and End Results-Medicare database diagnosed with stage IV colon cancer January 1, 1991 to December 31, 2005, who were later hospitalized for bowel obstruction.
Main outcome measures: We describe outcomes after hospitalization and analyzed the associations between surgical treatment of obstruction and outcomes.
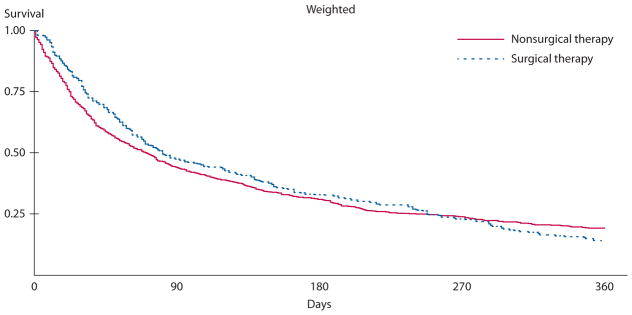
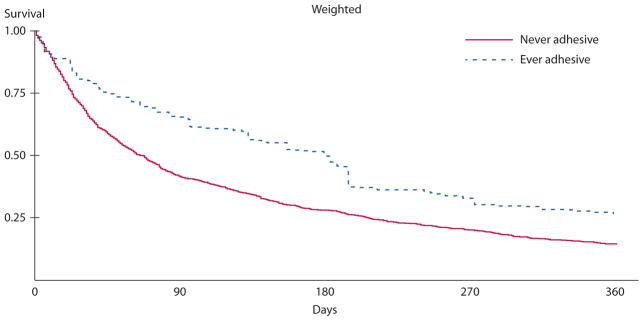
Results: Hospitalization for bowel obstruction occurred a median of 7.4 months after colon cancer diagnosis, and median survival after obstruction was approximately 2.5 months. Median hospitalization for obstruction was about 1 week and in-hospital mortality was 12.7%. Between discharge and death, 25% of patients were readmitted to the hospital at least once for obstruction, and, on average, patients lived 5 days out of the hospital for every day in the hospital between obstruction diagnosis and death. Survival was 3 times longer in those whose obstruction claims suggested an adhesive obstruction origin. In multivariable models, surgical compared with nonsurgical management was not associated with prolonged survival (p = 0.134).
Limitations: Use of an administrative database did not allow determination of quality of life or relief of obstruction as an outcome, nor could nonsurgical interventions, eg, endoscopic stenting or octreotide, be assessed.
Conclusions: In this population-based study of patients with stage IV colon cancer who had bowel obstruction, overall survival following obstruction was poor irrespective of treatment. Universally poor outcomes suggest that a diagnosis of obstruction in the setting of advanced colon cancer should be considered a preterminal event.
Figures
References
-
- Ripamonti C, Twycross R, Baines M, et al. Working Group of the European Association for Palliative Care. Clinical-practice recommendations for the management of bowel obstruction in patients with end-stage cancer. Support Care Cancer. 2001;9:223–233. - PubMed
-
- Feuer DJ, Broadley KE, Shepherd JH, Barton DP. Systematic review of surgery in malignant bowel obstruction in advanced gynecological and gastrointestinal cancer. The Systematic Review Steering Committee. Gynecol Oncol. 1999;75:313–322. - PubMed
-
- Pothuri B, Vaidya A, Aghajanian C, Venkatraman E, Barakat RR, Chi DS. Palliative surgery for bowel obstruction in recurrent ovarian cancer: an updated series. Gynecol Oncol. 2003;89:306–313. - PubMed
-
- Lee HJ, Hong SP, Cheon JH, et al. Long-term outcome of palliative therapy for malignant colorectal obstruction in patients with unresectable metastatic colorectal cancers: endoscopic stenting versus surgery. Gastrointest Endosc. 2011;73:535–542. - PubMed
-
- Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004;99:2051–2057. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
