

Rituximab is a safe and effective long-term treatment for children with steroid and calcineurin inhibitor-dependent idiopathic nephrotic syndrome
- PMID: 23739238
- PMCID: PMC3816123
- DOI: 10.1038/ki.2013.211
Rituximab is a safe and effective long-term treatment for children with steroid and calcineurin inhibitor-dependent idiopathic nephrotic syndrome
Abstract
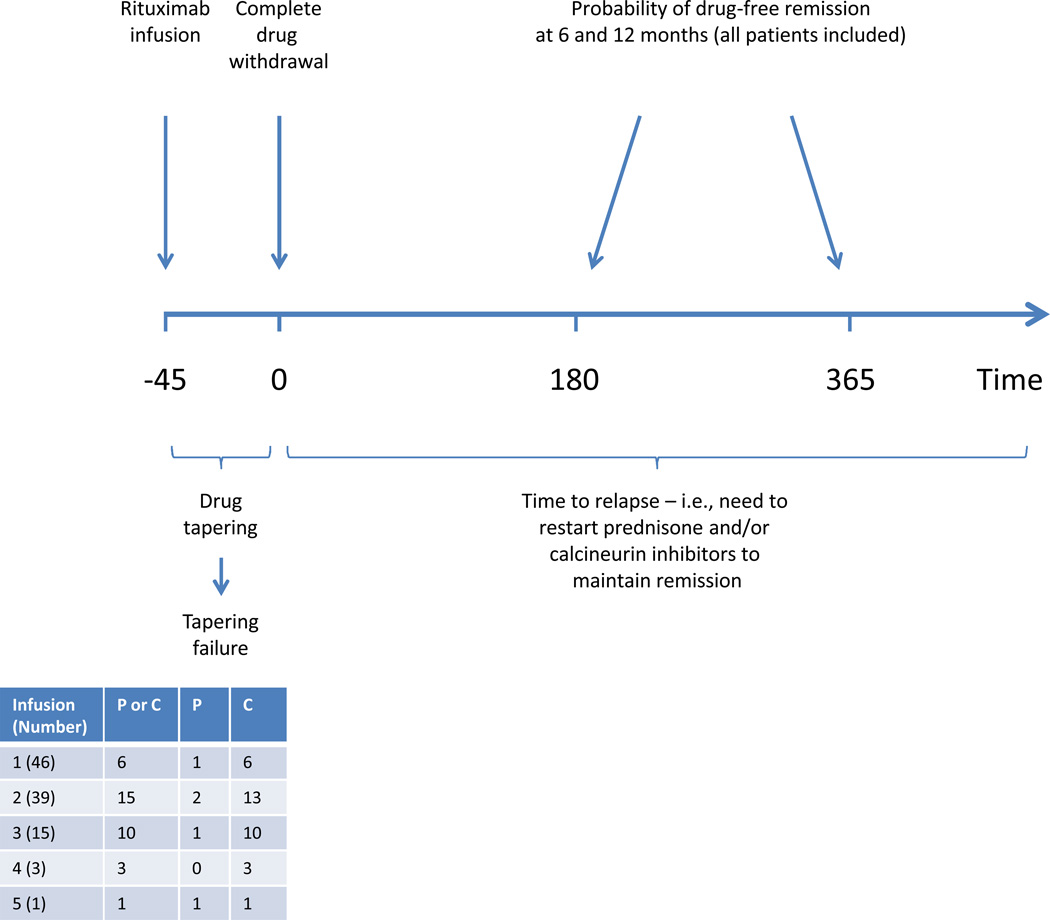
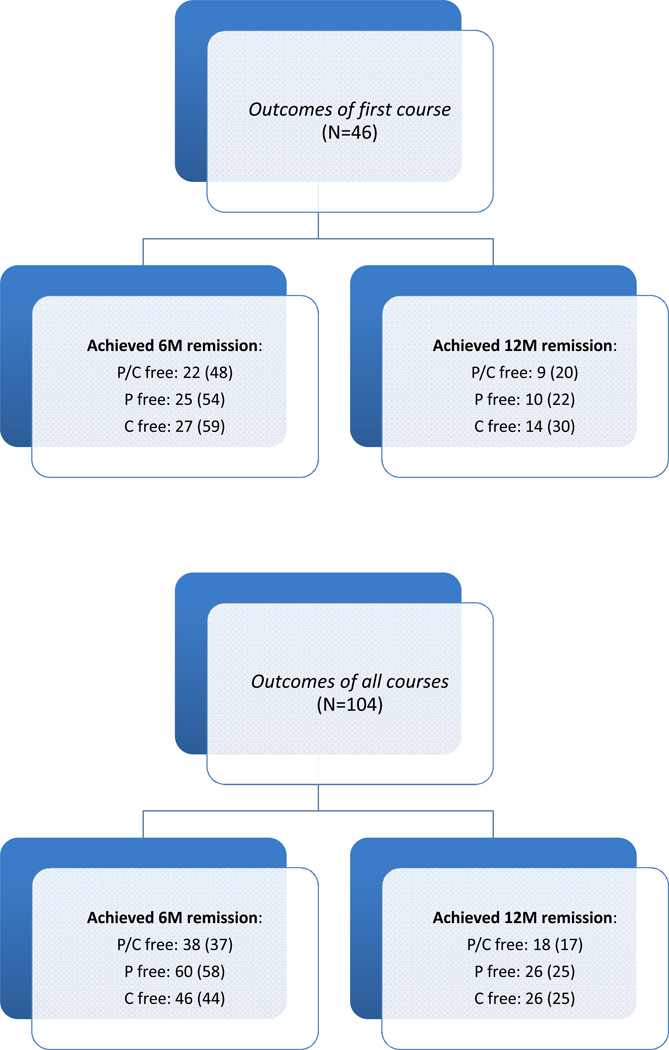
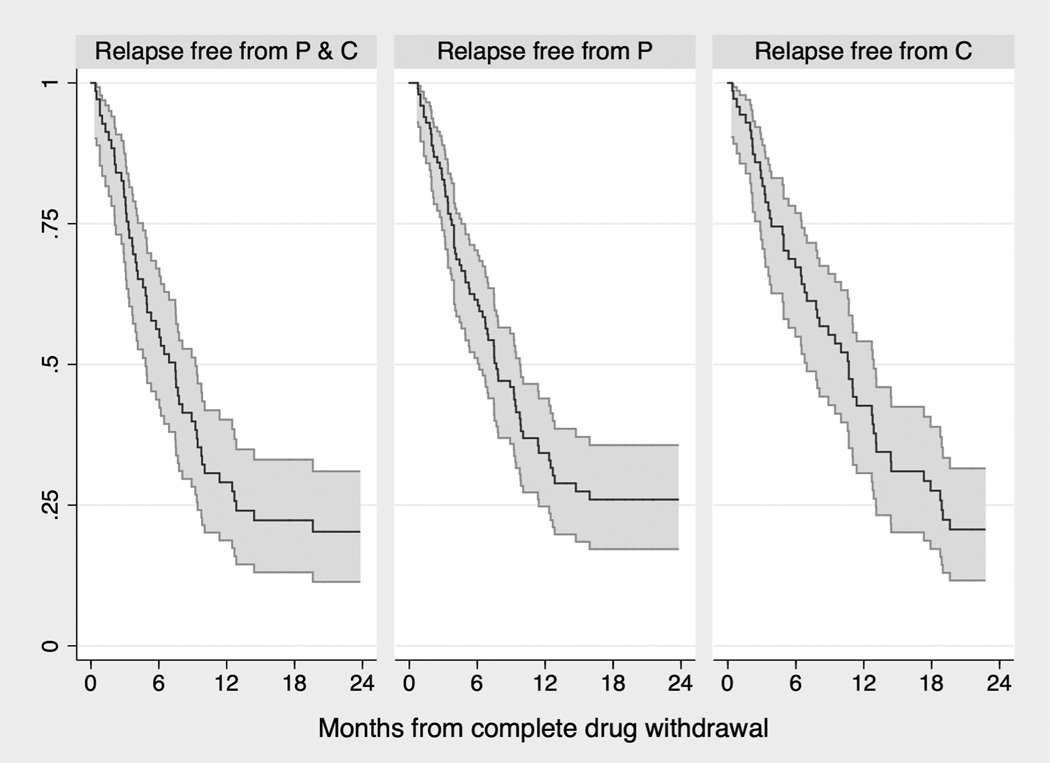
In children with idiopathic nephrotic syndrome, rituximab can maintain short-term remission with withdrawal of prednisone and calcineurin inhibitors. Long-term effects including the number of repeated infusions to maintain remission are unknown. To test this, we treated 46 consecutive children with idiopathic nephrotic syndrome lasting for at least 1 year (mean 6.3 years), maintained in remission with oral prednisone and calcineurin inhibitors. They received 1-5 rituximab courses during a median follow-up of 3 years. Oral agents were tapered after each infusion, and completely withdrawn within 45 days. Rituximab was well tolerated. Six-month probabilities of remission were 48% after the first infusion and 37% after subsequent infusions. One- and 2-year-remission probabilities were, respectively, 20 and 10%. Median time intervals between complete oral-agent withdrawal and relapse were 5.6 and 8.5 months, respectively, following the first and subsequent courses. The time to reconstitution of CD20 cells correlated with the duration of remission, but was not associated with variation in FcyR, CD20, or SMPDL-3B polymorphisms. Podocyte Src phosphorylation was normal. Thus, rituximab can be safely and repeatedly used as a prednisone and calcineurin inhibitor-sparing therapy in a considerable proportion of children with dependent forms of idiopathic nephrotic syndrome. Further study is needed to identify patients who will benefit most from rituximab therapy.
Conflict of interest statement
Figures
Comment in
-
Nephrotic syndrome: Rituximab in childhood steroid-dependent nephrotic syndrome.Nat Rev Nephrol. 2013 Oct;9(10):562-3. doi: 10.1038/nrneph.2013.153. Epub 2013 Aug 13. Nat Rev Nephrol. 2013. PMID: 23938594 No abstract available.
References
-
- Braden GL, Mulhern JG, O'Shea MH, Nash SV, et al. Changing incidence of glomerular diseases in adults. Am J Kidney Dis. 2000;35:878–883. - PubMed
-
- Trompeter RS, Lloyd BW, Hicks J, White RH, et al. Long-term outcome for children with minimal-change nephrotic syndrome. Lancet. 1985;1:368–370. - PubMed
-
- Ponticelli C, Rizzoni G, Edefonti A, Altieri P, et al. A randomized trial of cyclosporine in steroid-resistant idiopathic nephrotic syndrome. Kidney Int. 1993;43:1377–1384. - PubMed
-
- Ghiggeri GM, Catarsi P, Scolari F, Caridi G, et al. Cyclosporine in patients with steroid-resistant nephrotic syndrome: an open-label, nonrandomized, retrospective study. Clin Ther. 2004;26:1411–1418. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
