

Changes in circulating biomarkers of muscle atrophy, inflammation, and cartilage turnover in patients undergoing anterior cruciate ligament reconstruction and rehabilitation
- PMID: 23739685
- PMCID: PMC4086614
- DOI: 10.1177/0363546513490651
Changes in circulating biomarkers of muscle atrophy, inflammation, and cartilage turnover in patients undergoing anterior cruciate ligament reconstruction and rehabilitation
Abstract
Background: After anterior cruciate ligament (ACL) reconstruction, there is significant atrophy of the quadriceps muscles that can limit full recovery and place athletes at risk for recurrent injuries with return to play. The cause of this muscle atrophy is not fully understood.
Hypothesis: Circulating levels of proatrophy, proinflammatory, and cartilage turnover cytokines and biomarkers would increase after ACL reconstruction.
Study design: Descriptive laboratory study.
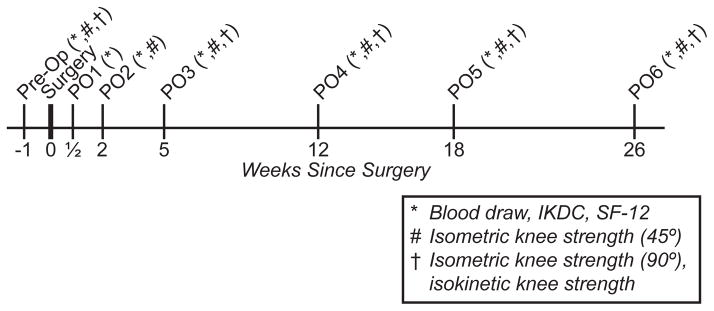
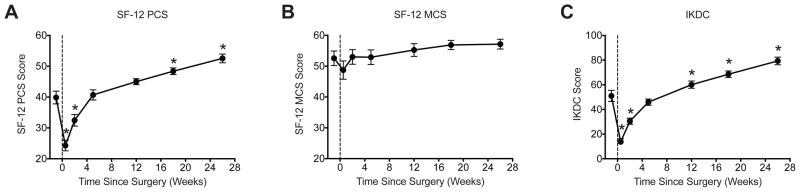
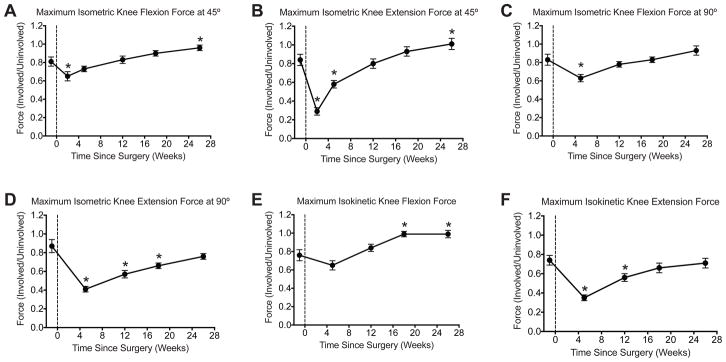
Methods: Patients (N = 18; mean age, 28 ± 2.4 years) underwent surgical reconstruction of the ACL after a noncontact athletic injury. Circulating levels of biomarkers were measured along with Short Form-12, International Knee Documentation Committee, and objective knee strength measures preoperatively and at 6 postoperative visits. Differences were tested using repeated-measures 1-way analysis of variance.
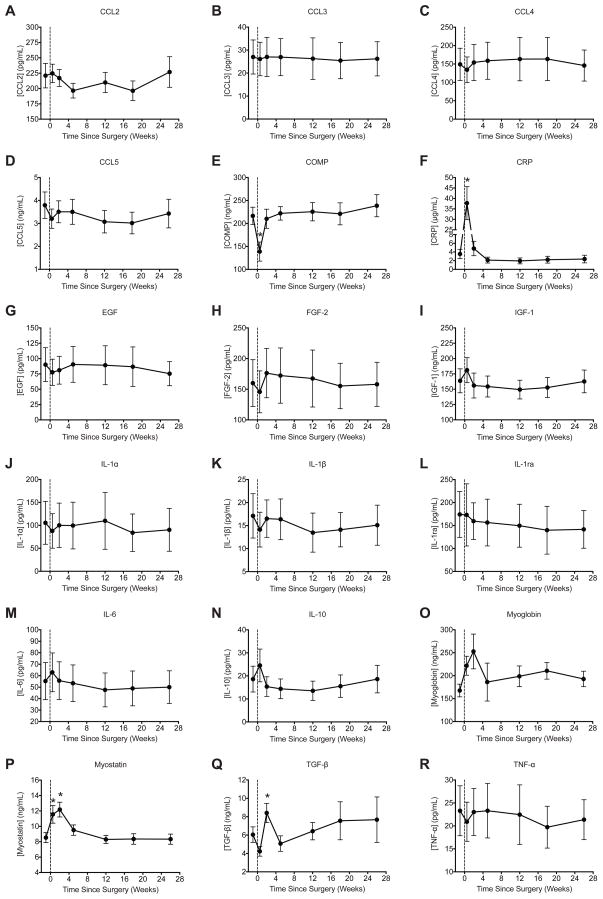
Results: Myostatin, TGF-β, and C-reactive protein levels were significantly increased in the early postoperative period and returned to baseline. Cartilage oligomeric matrix protein levels decreased immediately after surgery and then returned to baseline. CCL2, CCL3, CCL4, CCL5, EGF, FGF-2, IGF-1, IL-10, IL-1α, IL-1β, IL-1ra, IL-6, myoglobin, and TNF-α were not different over the course of the study.
Conclusion: An increase in potent atrophy-inducing cytokines and corresponding changes in knee strength and functional scores were observed after ACL reconstruction.
Clinical relevance: Although further studies are necessary, the therapeutic inhibition of myostatin may help prevent the muscle atrophy that occurs after ACL reconstruction and provide an accelerated return of patients to sport.
Keywords: ACL reconstruction; C-reactive protein; cartilage oligomeric matrix protein; muscle atrophy; myostatin; transforming growth factor-β.
Figures
References
-
- Anderson AF, Irrgang JJ, Kocher MS, Mann BJ, Harrast JJ, Committee I. The International Knee Documentation Committee Subjective Knee Evaluation Form: normative data. Am J Sports Med. 2006;34(1):128–135. - PubMed
-
- Attie KM, Borgstein NG, Yang Y, et al. A single ascending-dose study of muscle regulator ACE-031 in healthy volunteers. Muscle & nerve. 2012 - PubMed
-
- Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nichols CE. Treatment of anterior cruciate ligament injuries, part 2. American Journal of Sports Medicine. 2005;33(11):1751–1767. - PubMed
-
- Beynnon BD, Uh BS, Johnson RJ, et al. Rehabilitation after anterior cruciate ligament reconstruction: a prospective, randomized, double-blind comparison of programs administered over 2 different time intervals. American Journal of Sports Medicine. 2005;33(3):347–359. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
