

Noninvasive estimation of raised intracranial pressure using ocular ultrasonography in liver transplant recipients with acute liver failure -A report of two cases-
- PMID: 23741570
- PMCID: PMC3668109
- DOI: 10.4097/kjae.2013.64.5.451
Noninvasive estimation of raised intracranial pressure using ocular ultrasonography in liver transplant recipients with acute liver failure -A report of two cases-
Abstract
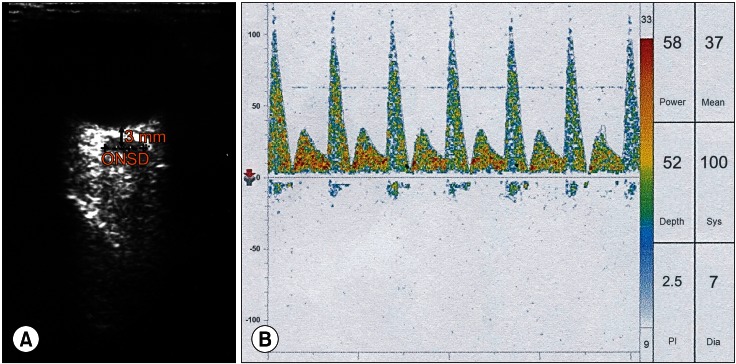
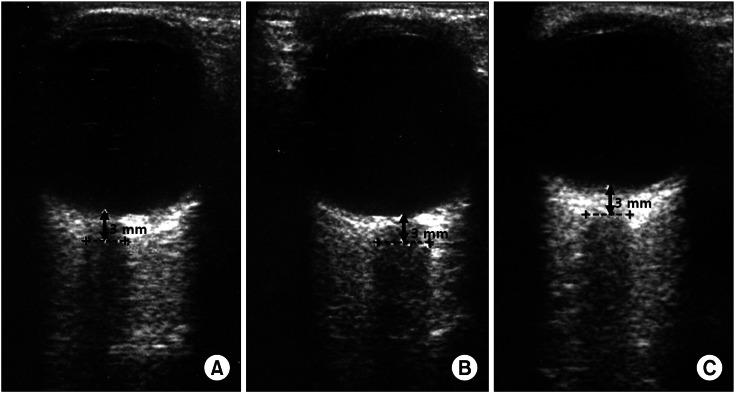
Intracranial pressure (ICP) monitoring is an important issue for liver transplant recipients, since increased ICP is associated with advanced hepatic encephalopathy or graft reperfusion during liver transplantation. Invasive monitoring of ICP is known as a gold standard method, but it can provoke bleeding and infection; thus, its use is a controversial issue. Studies have shown that optic nerve sheath diameter > 5 mm by ocular ultrasonography is useful for evaluating ICP > 20 mmHg noninvasively in many clinical settings. In this case report, we present experiences of using ocular ultrasound as a diagnostic tool that could detect changes in ICP noninvasively during liver transplantation.
Keywords: Intracranial pressure; Liver transplantation; Ocular ultrasonography.
Figures
Similar articles
-
Perioperative monitoring of intracranial pressure using optic nerve sheath diameter in paediatric liver transplantation.Indian J Anaesth. 2018 Nov;62(11):892-895. doi: 10.4103/ija.IJA_104_18. Indian J Anaesth. 2018. PMID: 30532327 Free PMC article.
-
Detection and monitoring of intracranial pressure dysregulation in liver failure by ultrasound.Transplantation. 2000 Jul 27;70(2):392-5. doi: 10.1097/00007890-200007270-00029. Transplantation. 2000. PMID: 10933171
-
Ultrasonographic optic nerve sheath diameter is correlated with arterial carbon dioxide concentration during reperfusion in liver transplant recipients.Transplant Proc. 2013 Jul-Aug;45(6):2272-6. doi: 10.1016/j.transproceed.2012.12.032. Epub 2013 Jul 17. Transplant Proc. 2013. PMID: 23871183
-
Raised intracranial pressure in hepatic encephalopathy.Indian J Gastroenterol. 2003 Dec;22 Suppl 2:S62-5. Indian J Gastroenterol. 2003. PMID: 15025259 Review.
-
Optic nerve sheath diameter: present and future perspectives for neurologists and critical care physicians.Neurol Sci. 2019 Dec;40(12):2447-2457. doi: 10.1007/s10072-019-04015-x. Epub 2019 Jul 31. Neurol Sci. 2019. PMID: 31367861 Review.
Cited by
-
Neuromuscular ultrasound of cranial nerves.J Clin Neurol. 2015 Apr;11(2):109-21. doi: 10.3988/jcn.2015.11.2.109. J Clin Neurol. 2015. PMID: 25851889 Free PMC article. Review.
-
The Role of Transocular Ultrasound in the Assessment of Neurotoxicity-Related Encephalopathy in Mushroom Poisoning.Turk J Anaesthesiol Reanim. 2020 Feb;48(1):62-67. doi: 10.5152/TJAR.2019.37891. Epub 2019 Oct 8. Turk J Anaesthesiol Reanim. 2020. PMID: 32076682 Free PMC article.
-
Noninvasive monitoring intracranial pressure - A review of available modalities.Surg Neurol Int. 2017 Apr 5;8:51. doi: 10.4103/sni.sni_403_16. eCollection 2017. Surg Neurol Int. 2017. PMID: 28480113 Free PMC article. Review.
-
Optic nerve ultrasound for fluid status assessment in patients with severe preeclampsia.Radiol Oncol. 2018 Nov 26;52(4):377-382. doi: 10.2478/raon-2018-0047. Radiol Oncol. 2018. PMID: 30511937 Free PMC article.
-
Multimodal brain monitoring in fulminant hepatic failure.World J Hepatol. 2016 Aug 8;8(22):915-23. doi: 10.4254/wjh.v8.i22.915. World J Hepatol. 2016. PMID: 27574545 Free PMC article. Review.
References
-
- Ede RJ, Williams RW. Hepatic encephalopathy and cerebral edema. Semin Liver Dis. 1986;6:107–118. - PubMed
-
- Detry O, Arkadopoulos N, Ting P, Kahaku E, Margulies J, Arnaout W, et al. Intracranial pressure during liver transplantation for fulminant hepatic failure. Transplantation. 1999;67:767–770. - PubMed
-
- Keays R, Potter D, O'Grady J, Peachey T, Alexander G, Williams R. Intracranial and cerebral perfusion pressure changes before, during and immediately after orthotopic liver transplantation for fulminant hepatic failure. Q J Med. 1991;79:425–433. - PubMed
-
- Steadman RH, Van Rensburg A, Kramer DJ. Transplantation for acute liver failure: perioperative management. Curr Opin Organ Transplant. 2010;15:368–373. - PubMed
-
- Lang EW, Chesnut RM. Intracranial pressure. Monitoring and management. Neurosurg Clin N Am. 1994;5:573–605. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
