Optimal timing of surgery after neoadjuvant chemoradiation therapy in locally advanced rectal cancer
- PMID: 23741691
- PMCID: PMC3671002
- DOI: 10.4174/jkss.2013.84.6.338
Optimal timing of surgery after neoadjuvant chemoradiation therapy in locally advanced rectal cancer
Abstract
Purpose: The optimal time between neoadjuvant chemoradiotherapy (CRT) and surgery for rectal cancer has been debated. This study evaluated the influence of this interval on oncological outcomes.
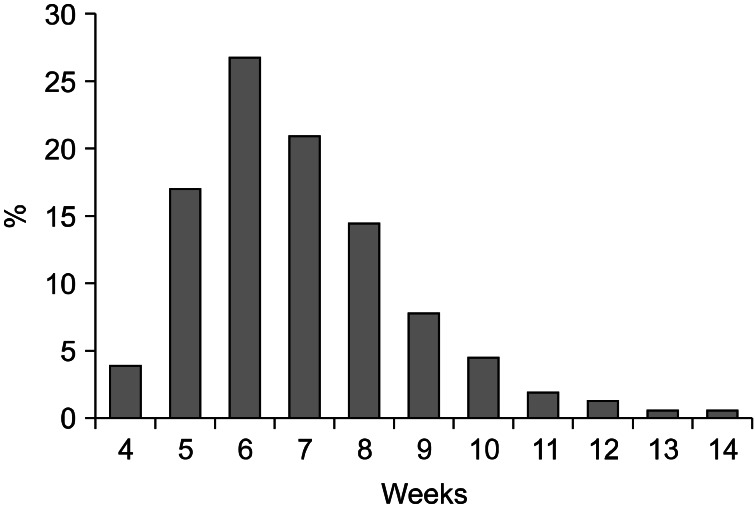
Methods: We compared postoperative complications, pathological downstaging, disease recurrence, and survival in patients with locally advanced rectal cancer who underwent surgical resection <8 weeks (group A, n = 105) to those who had surgery ≥8 weeks (group B, n = 48) after neoadjuvant CRT.
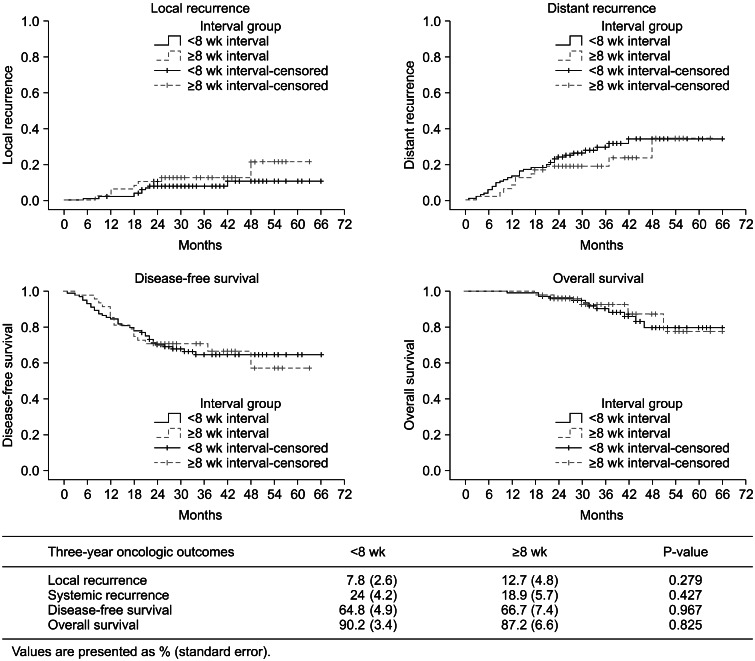
Results: Of 153 patients, 117 (76.5%) were male and 36 (23.5%) were female. Mean age was 57.8 years (range, 28 to 79 years). There was no difference in the rate of sphincter preserving surgery between the two groups (group A, 82.7% vs. group B, 77.6%; P = 0.509). The longer interval group had decreased postoperative complications, although statistical significance was not reached (group A, 28.8% vs. group B, 14.3%; P = 0.068). A total of 111 (group A, 75 [71.4%] and group B, 36 [75%]) patients were downstaged and 26 (group A, 17 [16.2%] and group B, 9 [18%]) achieved pathological complete response (pCR). There was no significant difference in the pCR rate (P = 0.817). The longer interval group experienced significant improvement in the nodal (N) downstaging rate (group A, 46.7% vs. group B, 66.7%; P = 0.024). The local recurrence (P = 0.279), distant recurrence (P = 0.427), disease-free survival (P = 0.967), and overall survival (P = 0.825) rates were not significantly different.
Conclusion: It is worth delaying surgical resection for 8 weeks or more after completion of CRT as it is safe and is associated with higher nodal downstaging rates.
Keywords: Chemoradiotherapy; Neoadjuvant therapy; Preoperative period; Rectal neoplasm; Surgery.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- de Campos-Lobato LF, Geisler DP, da Luz Moreira A, Stocchi L, Dietz D, Kalady MF. Neoadjuvant therapy for rectal cancer: the impact of longer interval between chemoradiation and surgery. J Gastrointest Surg. 2011;15:444–450. - PubMed
-
- Lim SB, Choi HS, Jeong SY, Kim DY, Jung KH, Hong YS, et al. Optimal surgery time after preoperative chemoradiotherapy for locally advanced rectal cancers. Ann Surg. 2008;248:243–251. - PubMed
-
- Pahlman L. Optimal timing of surgery after preoperative chemoradiotherapy for rectal cancer. Nat Clin Pract Oncol. 2009;6:128–129. - PubMed
-
- Habr-Gama A, Perez RO, Proscurshim I, Nunes Dos Santos RM, Kiss D, Gama-Rodrigues J, et al. Interval between surgery and neoadjuvant chemoradiation therapy for distal rectal cancer: does delayed surgery have an impact on outcome? Int J Radiat Oncol Biol Phys. 2008;71:1181–1188. - PubMed
-
- Colorectal Cancer Collaborative Group. Adjuvant radiotherapy for rectal cancer: a systematic overview of 8,507 patients from 22 randomised trials. Lancet. 2001;358:1291–1304. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials