

Perioperative outcomes of robotic versus laparoscopic hysterectomy for benign disease
- PMID: 23743379
- PMCID: PMC3662725
- DOI: 10.4293/108680812X13517013317914
Perioperative outcomes of robotic versus laparoscopic hysterectomy for benign disease
Abstract
Background and objectives: We compared the perioperative outcomes of hysterectomy performed by robotic (RH) versus laparoscopic (LH) routes for benign indications using the Dindo-Clavien scale for classification of the surgical complications.
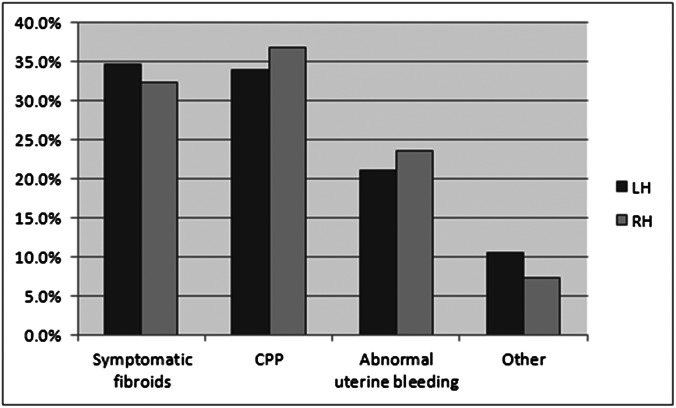
Methods: Retrospective chart review of all patients who underwent robotic (n=288) and laparoscopic (n=257) hysterectomies by minimally invasive surgeons at the University of Michigan from March 2001 until June 2010.
Results: Age, body mass index, operative time, and estimated blood loss were not statistically different between groups. The RH subgroup had a larger uterine weight (LH 186.4±130.6 g vs RH 234.9±193.9 g, P=.001), higher prevalence of severe adhesions (13.2% vs 23.3%, respectively, P=.003), and stage III-IV endometriosis (4.7% vs 15.3%, respectively, P<.05). There were no differences in the rates of Dindo-Clavien grade I, grade II, and grade III surgical complications between the RH and LH groups (9.7%, 13.2%, and 3.1%, respectively, in the RH group vs 6.2%, 9.3%, and 5.8%, respectively, in the LH group, P>.05). However, the rates of urinary tract infection were higher in the RH group (LH 2.7% vs RH 6.9%, P=.02), whereas the conversion to laparotomy rate was higher in the LH group (LH 6.2% vs RH 1.7%, P=.007).
Conclusions: Perioperative outcomes for laparoscopic and robotic hysterectomy for benign indications appear to be equivalent.
Figures
References
-
- Nieboer TE, Johnson N, Lethaby A, et al. Surgical approach to hysterectomy for benign gynaecological disease. Cohcrane Database Syst Rev. 2009;8:CD003677 - PubMed
-
- Farquhar CM, Steiner CA. Hysterectomy rates in the United States 1990–1997. Obstet Gynecol. 2002;99:229–234 - PubMed
-
- Wu JM, Wechter ME, Geller EJ, Nguyen TV, Visco AG. Hysterectomy rates in the United States, 2003. Obstet Gynecol. 2007;110:1091–1095 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical