

Comparison of robotic, laparoscopic, and abdominal myomectomy in a community hospital
- PMID: 23743382
- PMCID: PMC3662728
- DOI: 10.4293/108680812X13517013317473
Comparison of robotic, laparoscopic, and abdominal myomectomy in a community hospital
Abstract
Background and objectives: To evaluate the operative outcomes between robotic, laparoscopic, and abdominal myomectomies performed by a private gynecologic oncology practice in a suburban community hospital.
Methods: The medical records of 322 consecutive robotic, laparoscopic, and abdominal myomectomies performed from January 2007 through December 2009 were reviewed. The outcomes were collected from a retrospective review of patient medical records.
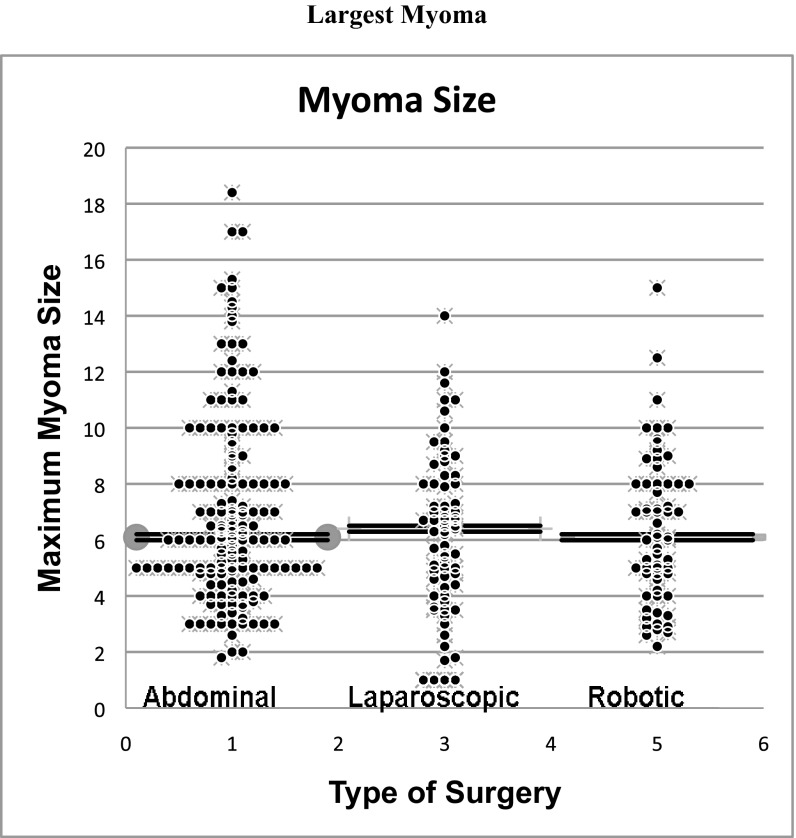
Results: Records for 14/322 (4.3%) patients were incomplete. Complete data were available for 308 patients, including 169 (54.9%) abdominal, 73 (23.7%) laparoscopic, and 66 (21.4%) robotic-assisted laparoscopic myomectomies. Patients were similar in age, body mass index, parity, and previous abdominopelvic surgery. Median operative time for robotic surgery (140 min) was significantly longer (P<.005) compared to laparoscopic (70 min) and abdominal (72 min) myomectomies. Robotic and laparoscopic myomectomies had significantly less estimated blood loss and hospital stay compared to abdominal myomectomies. There was no significant difference in complications or in the median size of the largest myoma removed between the different modalities. However, the median aggregate weight of myomas removed abdominally (200g; range, 1.4 to 2682) was significantly larger than that seen laparoscopically (115g; range, 1 to 602) and robotically (129g; range 9.4 to 935). Postoperative transfusion was significantly less frequent in robotic myomectomies compared to laparoscopic and abdominal myomectomies.
Conclusion: While robotic-assisted laparoscopic myomectomies had longer operative times, laparoscopic and robotic assisted laparoscopic myomectomies demonstrated shorter hospital stays, less blood loss, and fewer transfusions than abdominal myomectomies. Robotic myomectomy offers a minimally invasive alternative for management of symptomatic myoma in a community hospital setting.
Figures
References
-
- Agdi M, Tulandi T. Minimally invasive approach for myomectomy. Semin Reprod Med. 2010;28(3):228–234 - PubMed
-
- Bonney V. The techniques and results of myomectomy. Lancet. 1931;220:171–177
-
- Babaknia A, Rock JA, Jones HW., Jr Pregnancy success following abdominal myomectomy for infertility. Fertil Steril. 1978;30(6):644–647 - PubMed
-
- Parker WH. Uterine myomas: management. Fertil Steril. 2007;88(2):255–271 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical