

Review
doi: 10.1038/bjc.2013.177.
Epub 2013 Jun 6.
The benefits and harms of breast cancer screening: an independent review
Affiliations
- PMID: 23744281
- PMCID: PMC3693450
- DOI: 10.1038/bjc.2013.177
Item in Clipboard
Review
The benefits and harms of breast cancer screening: an independent review
Br J Cancer.
.
No abstract available
Figures
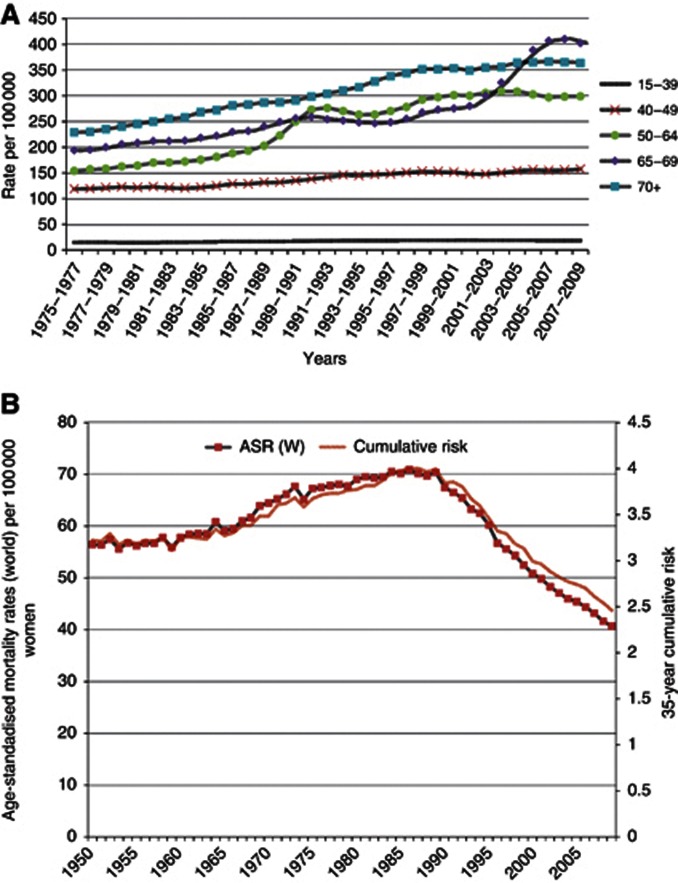
(A) European age-standardised incidence rates per 1 00 000 population, females, by age, Great Britain. (B) Breast cancer mortality at ages 35–69, UK, 1950–2009 (World Health Organization, 2012).
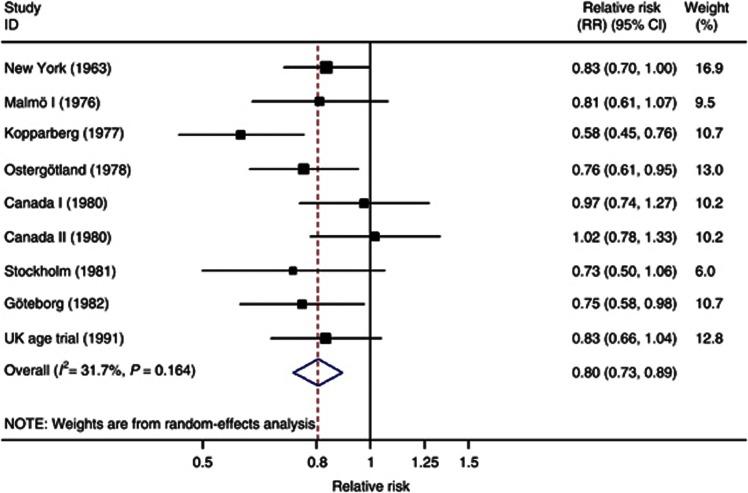
Meta-analysis of the breast cancer screening trials: RR of breast cancer mortality after 13 years of follow-up. Adapted from the Cochrane Review (Gøtzsche and Nielsen, 2011). Note: Malmö II is excluded because follow-up approximating 13 years was not available; the Swedish Two County (Kopparberg and Östergötland) and Canada I and II trials are split into their component parts; the Edinburgh trial is excluded because of severe imbalances between randomised groups.
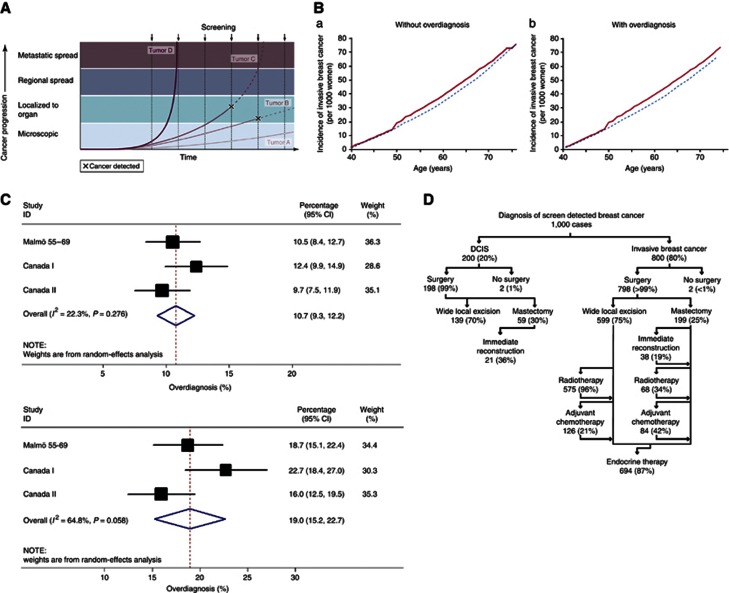
(A) Varying screen detection capability in relation to tumour growth rate (copied from Esserman et al, 2009). (B) Hypothetical cumulative incidence of breast cancer without (left) or with (right) overdiagnosis based on screening women between 50–68 years (copied from Biesheuvel et al, 2007; red line shows screened women and blue line unscreened women). (C) Meta-analysis of estimates of overdiagnosis: (a) excess cancers as a proportion of cancers diagnosed over whole follow-up period in women invited for screening, (b): excess cancers as a proportion of cancers diagnosed during screening period in women invited for screening. (D) Consequences of overdiagnosis.
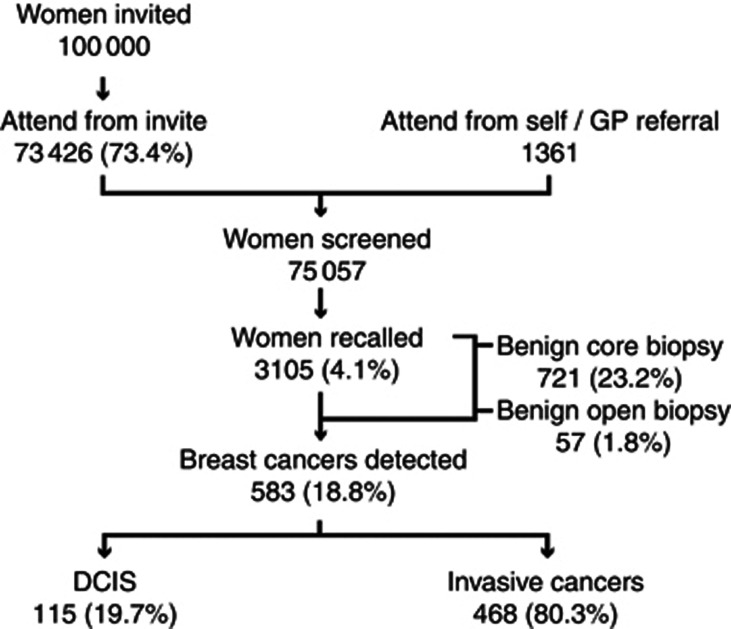
The assessment process. Overall cancer detection rate is 583/75 057=7.8 cancers per 1000 women screened. Of the 3105 women recalled, 583 (18.7%) will be diagnosed with invasive or in situ cancer. Data extracted for women aged 50–70 for year 2009/10 (NHS Breast Screening Programme, 2011; NHS Breast Screening Programme & Association of Breast Surgery-West Midlands Cancer Intelligence Unit, 2012).
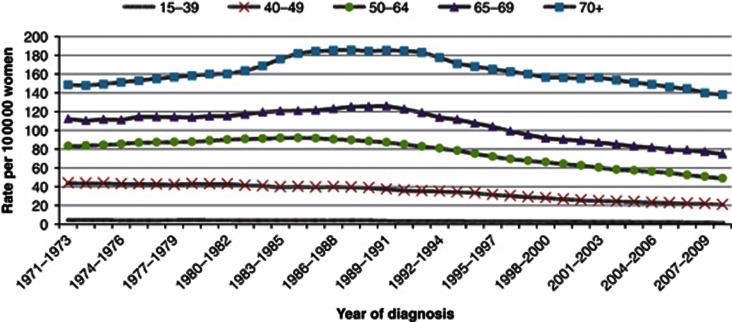
European age-standardised mortality rates, breast cancer, women, by age, UK 1971–2010. (Cancer Research UK, 2012).
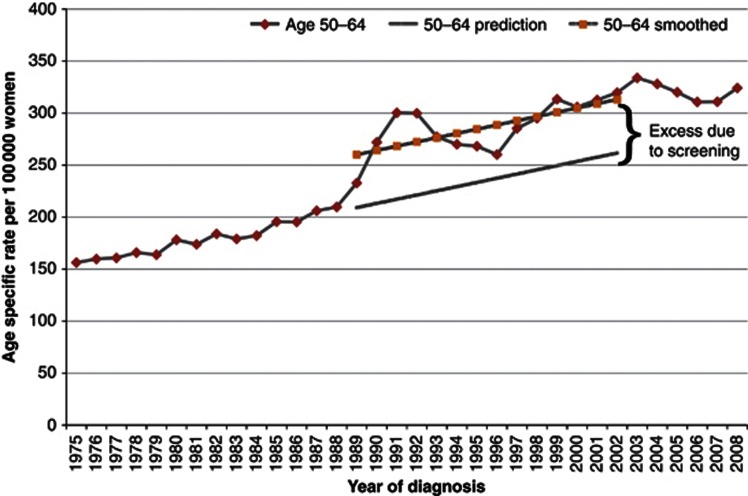
Breast cancer age-specific incidence rates, England 1975–2008. Description to include: breast cancer age-specific incidence rates, England 1975–2008, age 50–64 with expected, observed and smoothed data.
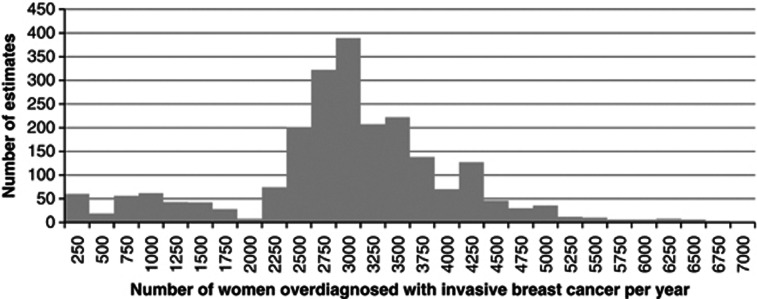
Histogram of the range of estimates.
Comment in
-
Mortality benefits and overdiagnosis estimates for women attending breast screening.Br J Cancer. 2013 Jun 11;108(11):2413-4. doi: 10.1038/bjc.2013.260. Epub 2013 Jun 6. Br J Cancer. 2013. PMID: 23744279 Free PMC article. No abstract available.
-
Breast cancer screening: time to target women at risk.Br J Cancer. 2013 Jun 11;108(11):2202-4. doi: 10.1038/bjc.2013.257. Epub 2013 Jun 6. Br J Cancer. 2013. PMID: 23744280 Free PMC article. No abstract available.
References
-
- Berry DA, Cronin KA, Plevritis SK, Fryback DG, Clarke l, Zelen M, Mandelblatt JS, Yakovlev AY, Habbema JD, Feuer EJ. Effect of screening and adjuvant therapy on mortality from breast cancer. N Engl J Med. 2005;353 (17:1784–1792. - PubMed
-
- Cancer Research UK 2012Breast Cancer Incidence Statistics.< http://info.cancerresearchuk.org/cancerstats/types/breast/incidence/#sex >(accessed 15 September 2012.
-
- Forrest P. Breast Cancer Screening - Report to the Health Ministers of England, Wales, Scotland and Northern Ireland. Department of Health and Social Security; 1986.
-
- Gotzsche PC, Nielsen M. Screening for breast cancer with mammography. Cochrane Database Syst Rev. 2011. p. CD001877. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
