

Timing of hemoconcentration during treatment of acute decompensated heart failure and subsequent survival: importance of sustained decongestion
- PMID: 23747773
- PMCID: PMC3892152
- DOI: 10.1016/j.jacc.2013.05.027
Timing of hemoconcentration during treatment of acute decompensated heart failure and subsequent survival: importance of sustained decongestion
Abstract
Objectives: This study sought to determine if the timing of hemoconcentration influences associated survival.
Background: Indicating a reduction in intravascular volume, hemoconcentration during the treatment of decompensated heart failure has been associated with reduced mortality. However, it is unclear if this survival advantage stems from the improved intravascular volume or if healthier patients are simply more responsive to diuretics. Rapid diuresis early in the hospitalization should similarly identify diuretic responsiveness, but hemoconcentration this early would not indicate euvolemia if extravascular fluid has not yet equilibrated.
Methods: Consecutive admissions at a single center with a primary discharge diagnosis of heart failure were reviewed (N = 845). Hemoconcentration was defined as an increase in both hemoglobin and hematocrit levels, then further dichotomized into early or late hemoconcentration by using the midway point of the hospitalization.
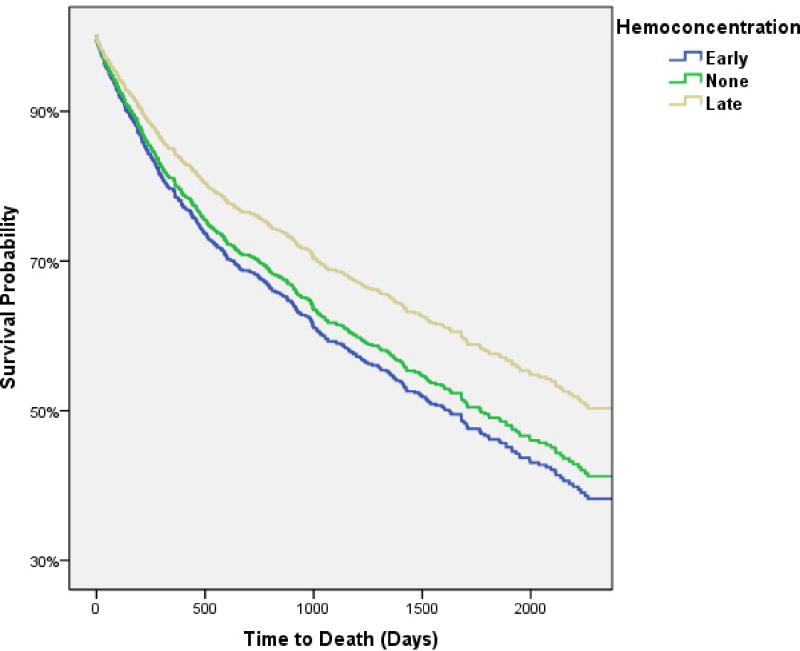
Results: Hemoconcentration occurred in 422 (49.9%) patients (41.5% early and 58.5% late). Patients with late versus early hemoconcentration had similar baseline characteristics, cumulative in-hospital loop diuretic administered, and worsening of renal function. However, patients with late hemoconcentration versus early hemoconcentration had higher average daily loop diuretic doses (p = 0.001), greater weight loss (p < 0.001), later transition to oral diuretics (p = 0.03), and shorter length of stay (p < 0.001). Late hemoconcentration conferred a significant survival advantage (hazard ratio: 0.74 [95% confidence interval: 0.59 to 0.93]; p = 0.009), whereas early hemoconcentration offered no significant mortality benefit (hazard ratio: 1.0 [95% confidence interval: 0.80 to 1.3]; p = 0.93) over no hemoconcentration.
Conclusions: Only hemoconcentration occurring late in the hospitalization was associated with improved survival. These results provide further support for the importance of achieving sustained decongestion during treatment of decompensated heart failure.
Keywords: ADHF; B-type natriuretic peptide; BNP; CI; HC; HR; Hct; Hgb; IQR; OR; WRF; acute decompensated heart failure; confidence interval; decompensated heart failure; eGFR; estimated glomerular filtration rate; hazard ratio; hematocrit; hemoconcentration; hemoglobin; interquartile range; mortality; odds ratio; worsening renal function.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures



References
-
- Gheorghiade M, Filippatos G, De Luca L, Burnett J. Congestion in acute heart failure syndromes: an essential target of evaluation and treatment. The American Journal of Medicine. 2006;119:S3–S10. - PubMed
-
- Adams KF, Jr, Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE) Am Heart J. 2005;149:209–16. - PubMed
-
- Schneditz D, Pogglitsch H, Horina J, Binswanger U. A blood protein monitor for the continuous measurement of blood volume changes during hemodialysis. Kidney Int. 1990;38:342–346. - PubMed
-
- Leypoldt JK, Cheung AK, Steuer RR, Harris DH, Conis JM. Determination of circulating blood volume by continuously monitoring hematocrit during hemodialysis. Journal of the American Society of Nephrology : JASN. 1995;6:214–219. - PubMed
-
- Boyle A, Sobotka PA. Redefining the therapeutic objective in decompensated heart failure: hemoconcentration as a surrogate for plasma refill rate. J Card Fail. 2006;12:247–249. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
