

Activation of inspiratory muscles via spinal cord stimulation
- PMID: 23751522
- PMCID: PMC3812328
- DOI: 10.1016/j.resp.2013.06.001
Activation of inspiratory muscles via spinal cord stimulation
Abstract
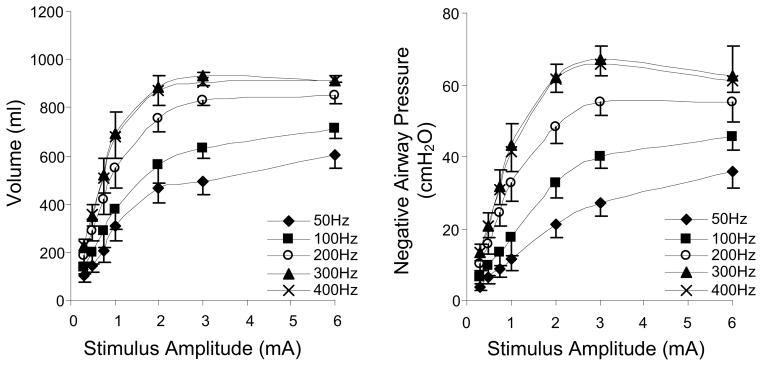
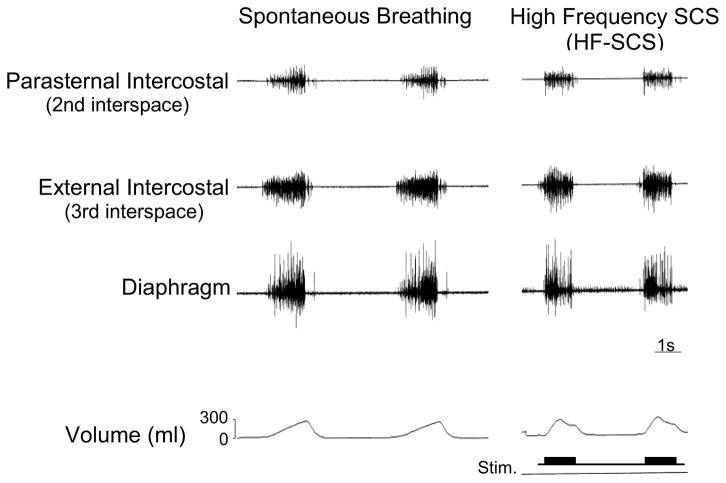
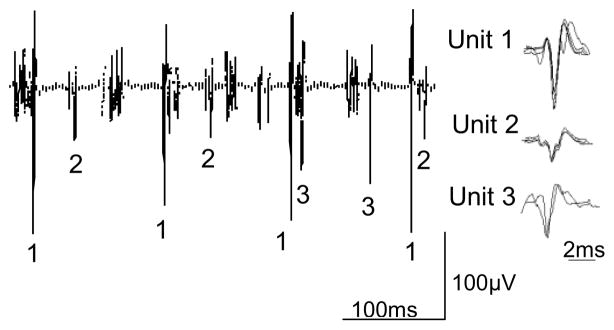
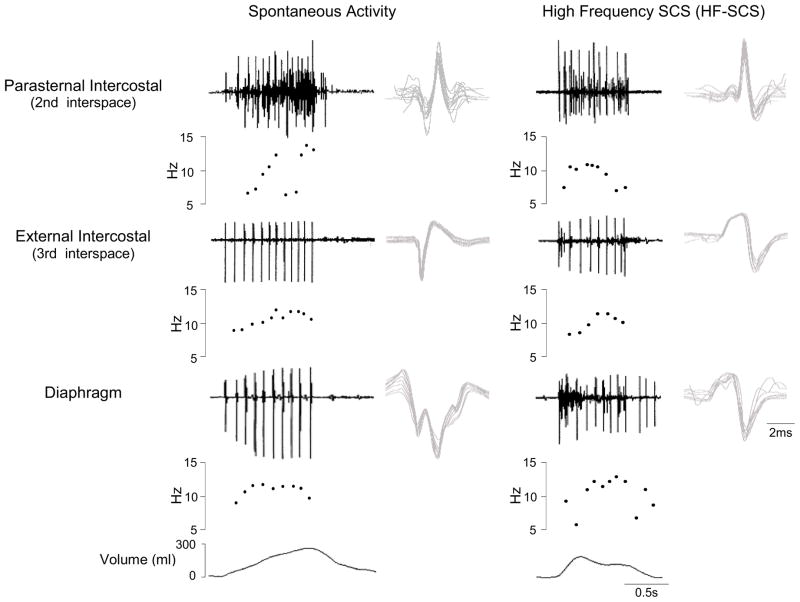
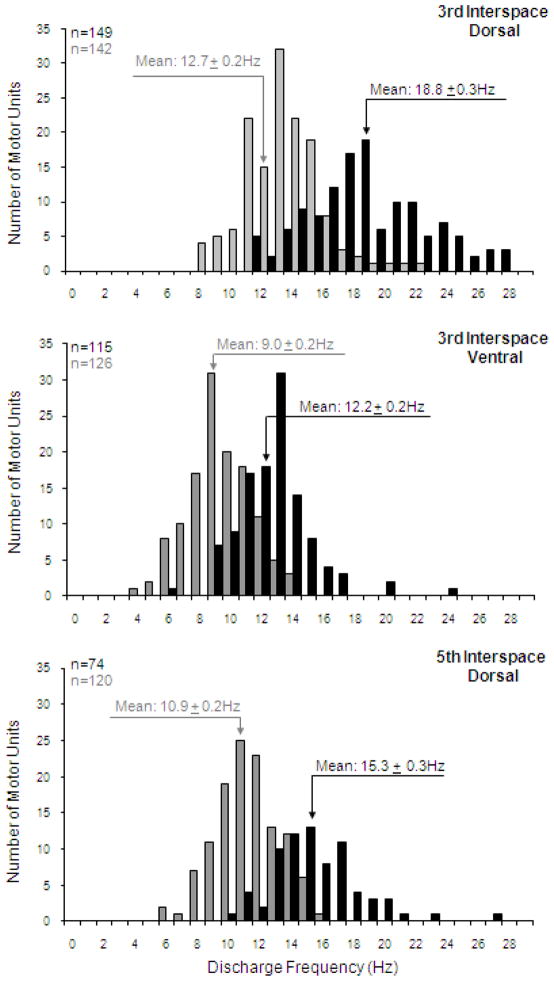
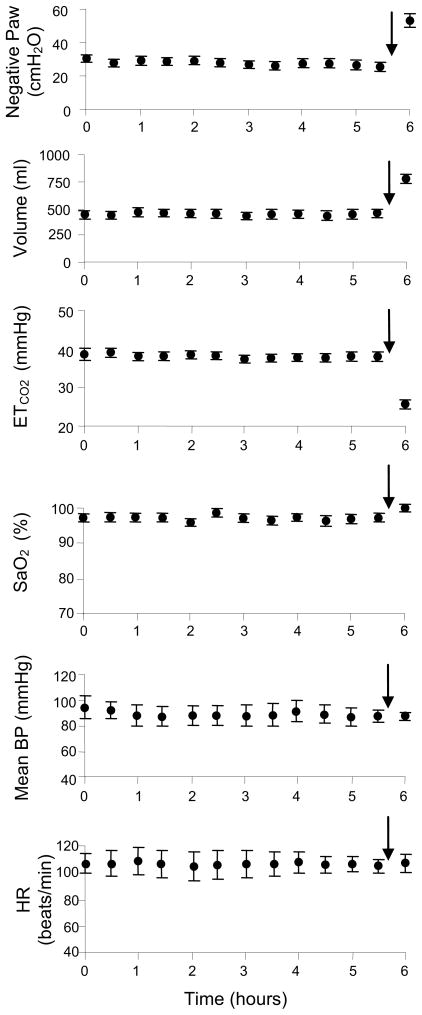
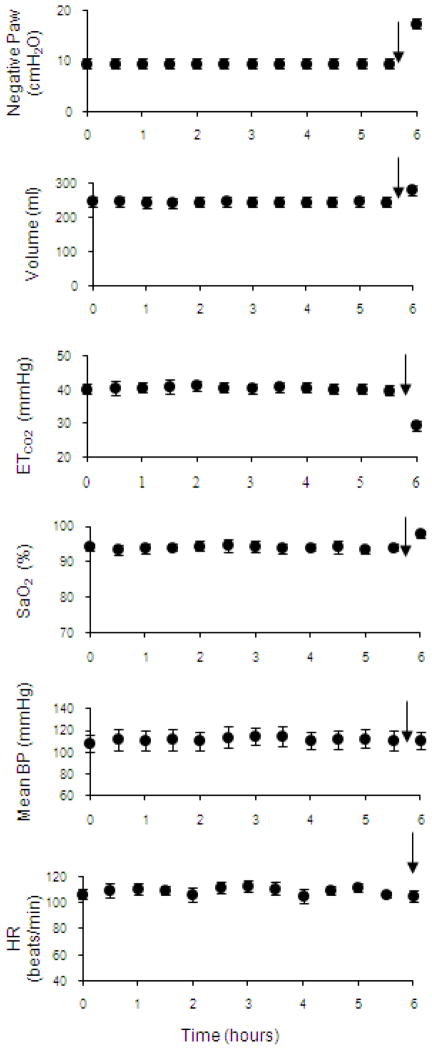
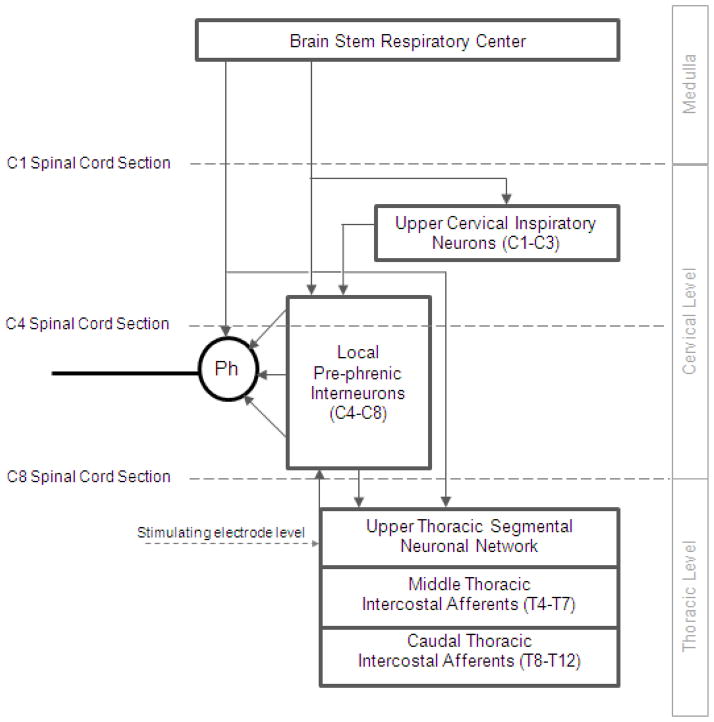
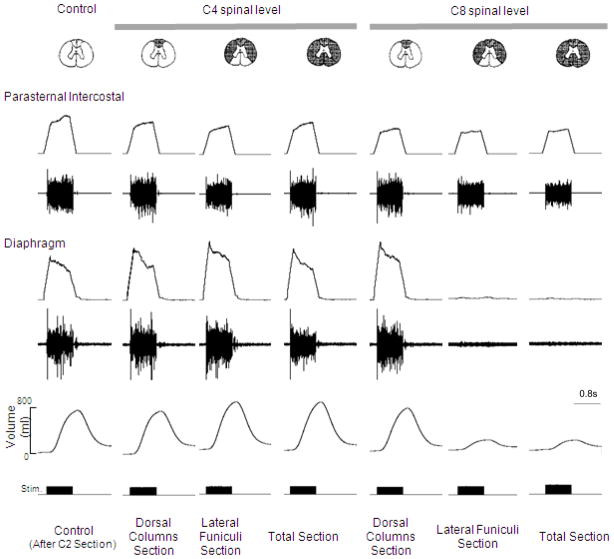
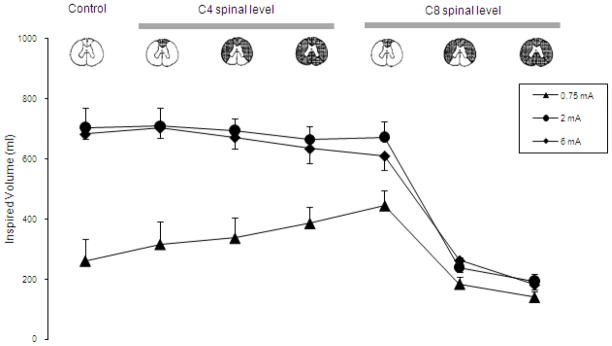
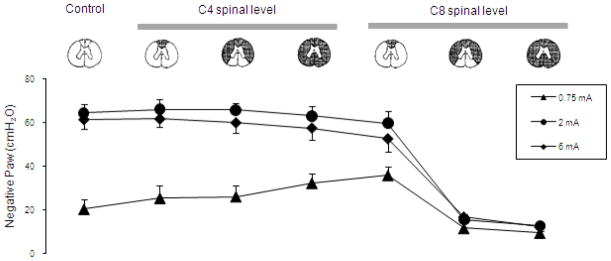
Diaphragm pacing is a clinically useful modality providing artificial ventilatory support in patients with ventilator dependent spinal cord injury. Since this technique is successful in providing full-time ventilatory support in only ~50% of patients, better methods are needed. In this paper, we review a novel method of inspiratory muscle activation involving the application of electrical stimulation applied to the ventral surface of the upper thoracic spinal cord at high stimulus frequencies (300 Hz). In an animal model, high frequency spinal cord stimulation (HF-SCS) results in synchronous activation of both the diaphragm and inspiratory intercostal muscles. Since this method results in an asynchronous pattern of EMG activity and mean peak firing frequencies similar to those observed during spontaneous breathing, HF-SCS is a more physiologic form of inspiratory muscle activation. Further, ventilation can be maintained on a long-term basis with repetitive stimulation at low stimulus amplitudes (<1 mA). These preliminary results suggest that HF-SCS holds promise as a more successful method of inspiratory muscle pacing.
Keywords: Diaphragm pacing; Inspiratory muscles; Spinal cord injury; Spinal cord stimulation.
Copyright © 2013 Elsevier B.V. All rights reserved.
Figures
Similar articles
-
Inspiratory muscle activation via ventral lower thoracic high-frequency spinal cord stimulation.J Appl Physiol (1985). 2019 Apr 1;126(4):977-983. doi: 10.1152/japplphysiol.01054.2018. Epub 2019 Feb 14. J Appl Physiol (1985). 2019. PMID: 30763163
-
Phrenic-to-intercostal reflex activity in response to high frequency spinal cord stimulation (HF-SCS).Respir Physiol Neurobiol. 2022 Dec;306:103962. doi: 10.1016/j.resp.2022.103962. Epub 2022 Sep 5. Respir Physiol Neurobiol. 2022. PMID: 36064141 Free PMC article.
-
Diaphragm activation via high frequency spinal cord stimulation in a rodent model of spinal cord injury.Exp Neurol. 2013 Sep;247:689-93. doi: 10.1016/j.expneurol.2013.03.006. Epub 2013 Mar 13. Exp Neurol. 2013. PMID: 23499833 Free PMC article.
-
The neural control of human inspiratory muscles.Prog Brain Res. 2014;209:295-308. doi: 10.1016/B978-0-444-63274-6.00015-1. Prog Brain Res. 2014. PMID: 24746054 Review.
-
Phrenic nerve stimulation in patients with spinal cord injury.Respir Physiol Neurobiol. 2009 Nov 30;169(2):200-9. doi: 10.1016/j.resp.2009.09.008. Epub 2009 Sep 26. Respir Physiol Neurobiol. 2009. PMID: 19786125 Review.
Cited by
-
Epidural Spinal Cord Stimulation for Spinal Cord Injury in Humans: A Systematic Review.J Clin Med. 2024 Feb 14;13(4):1090. doi: 10.3390/jcm13041090. J Clin Med. 2024. PMID: 38398403 Free PMC article. Review.
-
Closed-loop cervical epidural stimulation partially restores ipsilesional diaphragm EMG after acute C2 hemisection.Respir Physiol Neurobiol. 2024 Feb;320:104182. doi: 10.1016/j.resp.2023.104182. Epub 2023 Nov 1. Respir Physiol Neurobiol. 2024. PMID: 37923238 Free PMC article.
-
High-frequency epidural stimulation across the respiratory cycle evokes phrenic short-term potentiation after incomplete cervical spinal cord injury.J Neurophysiol. 2017 Oct 1;118(4):2344-2357. doi: 10.1152/jn.00913.2016. Epub 2017 Jun 14. J Neurophysiol. 2017. PMID: 28615341 Free PMC article.
-
High frequency spinal cord stimulation-New method to restore cough.Respir Physiol Neurobiol. 2016 Oct;232:54-6. doi: 10.1016/j.resp.2016.07.001. Epub 2016 Jul 6. Respir Physiol Neurobiol. 2016. PMID: 27395446 Free PMC article.
-
Regulation of Human Respiration by Electrical Stimulation.J Evol Biochem Physiol. 2022;58(6):1879-1891. doi: 10.1134/S0022093022060175. Epub 2022 Dec 22. J Evol Biochem Physiol. 2022. PMID: 36573159 Free PMC article.
References
-
- Acker MA, Mannion JD, Brown WE, Salmons S, Henriksson J, Bitto T, Gale DR, Hammond R, Stephenson LW. Canine diaphragm muscle after 1 yr of continuous electrical stimulation: its potential as a myocardial substitute. J Appl Physiol. 1987;62:1264–1270. - PubMed
-
- Adler D, Gonzalez-Bermejo J, Duguet A, Demoule A, Le Pimpec-Barthes F, Hurbault A, Morélot-Panzini C, Similowski T. Diaphragm pacing restores olfaction in tetraplegia. Eur Respir J. 2009;34:365–370. - PubMed
-
- Agostoni E, Mognoni P, Torri G, Agostoni AF. Static features of the passive rib cage and abdomen-diaphragm. J Appl Physiol. 1965;20:1187–1193.
-
- Ali A, Flageole H. Diaphragmatic pacing for the treatment of congenital central alveolar hypoventilation syndrome. J Pedatr Surg. 2008;43:792–796. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
