

Decreased relative diagnostic yield of esophagogastroduodenoscopy in children with gastroparesis
- PMID: 23751841
- PMCID: PMC4277878
- DOI: 10.1097/MCG.0b013e318299c8dd
Decreased relative diagnostic yield of esophagogastroduodenoscopy in children with gastroparesis
Abstract
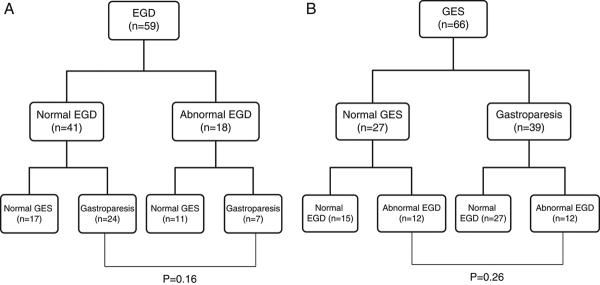
Background: Esophagogastroduodenoscopy (EGD) and gastric emptying scintigraphy (GES) are commonly performed in the evaluation of children with upper gastrointestinal symptoms. It has been presumed, but not clarified, that gastroparesis increases the likelihood of identifying abnormalities on EGD. We sought to determine whether the presence of gastroparesis influenced the diagnostic yield of EGD in children.
Methods: We conducted a retrospective chart review of children who underwent both an EGD and GES within 3 months of each other for evaluation of upper gastrointestinal symptoms (eg, abdominal pain). Clinical history (symptoms, comorbidities, medications, and surgical procedures), GES results, and EGD histology reports were captured.
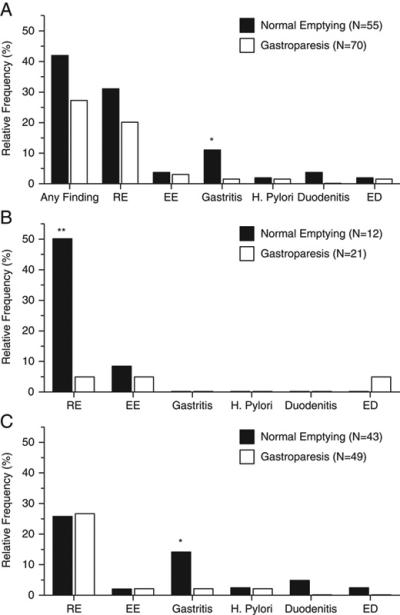
Results: A total of 125 children (46% female) were included, of whom, 70 (56%) had gastroparesis. Thirty-three (26%) children had liquid meal GES (1.2 ± 1.1 y of age, mean ± SD) and 92 (64%) had solid meal GES (12.4 ± 3.6 y of age). There was an overall trend toward a decreased frequency of biopsy abnormalities in those with gastroparesis (P=0.09). Those with gastroparesis identified through liquid meal GES were less likely to have reflux esophagitis on biopsy (P=0.002). Those with gastroparesis identified on solid meal GES were less likely to have gastritis (P=0.04). Symptoms, comorbidities, or medications were not predictive of GES or EGD results.
Conclusions: Children with gastroparesis may be less likely to have biopsy abnormalities identified on EGD in comparison to those without gastroparesis. Further prospective, larger, and multicenter studies are needed to validate our findings.
Figures
References
-
- Hasler WL. Gastroparesis: pathogenesis, diagnosis and management. Nat. Rev. Gastroenterol. Hepatol. 2011;8:438–453. - PubMed
-
- Parkman HP, Hasler WL, Fisher RS. American Gastroenterological Association technical review on the diagnosis and treatment of gastroparesis. Gastroenterology. 2004;127:1592–1622. - PubMed
-
- Abell TL, Camilleri M, Donohoe K, et al. Consensus recommendations for gastric emptying scintigraphy: a joint report of the American Neurogastroenterology and Motility Society and the Society of Nuclear Medicine. Am J Gastroenterol. 2008 Mar;103(3):753–63. Epub 2007 Nov 19. - PubMed
-
- Cassilly DW, Wang YR, Friedenberg FK, et al. Symptoms of gastroparesis: use of the gastroparesis cardinal symptom index in symptomatic patients referred for gastric emptying scintigraphy. Digestion. 2008;78(2-3):144–51. Epub 2008 Nov 22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
