

Shared care obesity management in 3-10 year old children: 12 month outcomes of HopSCOTCH randomised trial
- PMID: 23751902
- PMCID: PMC3677741
- DOI: 10.1136/bmj.f3092
Shared care obesity management in 3-10 year old children: 12 month outcomes of HopSCOTCH randomised trial
Abstract
Objective: To determine whether general practice surveillance for childhood obesity, followed by obesity management across primary and tertiary care settings using a shared care model, improves body mass index and related outcomes in obese children aged 3-10 years.
Design: Randomised controlled trial.
Setting: 22 family practices (35 participating general practitioners) and a tertiary weight management service (three paediatricians, two dietitians) in Melbourne, Australia.
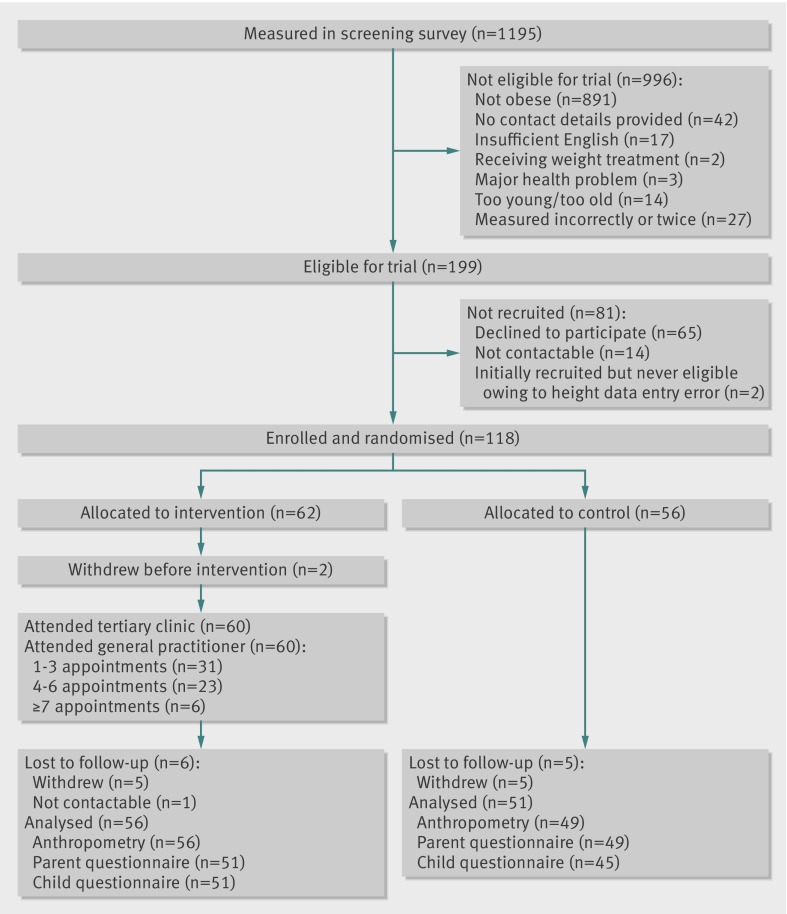
Participants: Children aged 3-10 years with body mass index above the 95th centile recruited through their general practice between July 2009 and April 2010.
Intervention: Children were randomly allocated to one tertiary appointment followed by up to 11 general practice consultations over one year, supported by shared care, web based software (intervention) or "usual care" (control). Researchers collecting outcome measurements, but not participants, were blinded to group assignment.
Main outcome measures: Children's body mass index z score (primary outcome), body fat percentage, waist circumference, physical activity, quality of diet, health related quality of life, self esteem, and body dissatisfaction and parents' body mass index (all 15 months post-enrolment).
Results: 118 (60 intervention, 56 control) children were recruited and 107 (91%) were retained and analysed (56 intervention, 51 control). All retained intervention children attended the tertiary appointment and their general practitioner for at least one (mean 3.5 (SD 2.5, range 1-11)) weight management consultation. At outcome, children in the two trial arms had similar body mass index (adjusted mean difference -0.1 (95% confidence interval -0.7 to 0.5; P=0.7)) and body mass index z score (-0.05 (-0.14 to 0.03); P=0.2). Similarly, no evidence was found of benefit or harm on any secondary outcome. Outcomes varied widely in the combined cohort (mean change in body mass index z score -0.20 (SD 0.25, range -0.97-0.47); 26% of children resolved from obese to overweight and 2% to normal weight.
Conclusions: Although feasible, not harmful, and highly rated by both families and general practitioners, the shared care model of primary and tertiary care management did not lead to better body mass index or other outcomes for the intervention group compared with the control group. Improvements in body mass index in both groups highlight the value of untreated controls when determining efficacy.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12608000055303.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures

References
-
- Olds T, Maher C, Zumin S, Peneau S, Lioret S, Castetbon K, et al. Evidence that the prevalence of childhood overweight is plateauing: data from nine countries. Int J Pediatr Obes 2011;6:342-60. - PubMed
-
- Australian Bureau of Statistics. National health survey: summary of results, 2007 - 2008. ABS, 2009.
-
- Australian Bureau of Statistics. Population by age and sex, Australian states and territories. Table 9. Estimated resident population by single year of age. 2007. www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/3201.0Jun%202007?OpenDocument.
-
- Singh AS, Mulder C, Twisk JW, van Mechelen W, Chinapaw MJ. Tracking of childhood overweight into adulthood: a systematic review of the literature. Obes Rev 2008;9:474-88. - PubMed
-
- Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes (Lond) 2011;35:891-8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous