

Adrenocortical carcinoma is a lynch syndrome-associated cancer
- PMID: 23752102
- PMCID: PMC3739861
- DOI: 10.1200/JCO.2012.48.0988
Adrenocortical carcinoma is a lynch syndrome-associated cancer
Erratum in
- J Clin Oncol. 2013 Oct 1;31(28):3612
Abstract
Purpose: Adrenocortical carcinoma (ACC) is an endocrine malignancy with a poor prognosis. The association of adult-onset ACC with inherited cancer predisposition syndromes is poorly understood. Our study sought to define the prevalence of Lynch syndrome (LS) among patients with ACC.
Patients and methods: One hundred fourteen patients with ACC were evaluated in a specialized endocrine oncology clinic and were prospectively offered genetic counseling and clinical genetics risk assessment (group 1). In addition, families with known mismatch repair (MMR) gene mutations that were recorded in the University of Michigan Cancer Genetics Registry were retrospectively reviewed for the presence of ACC (group 2). ACC tumors from patients with LS were tested for microsatellite instability and immunohistochemistry (IHC) to evaluate for MMR deficiency.
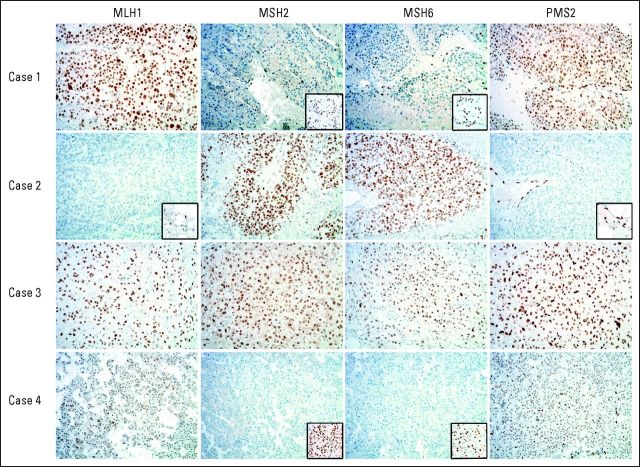
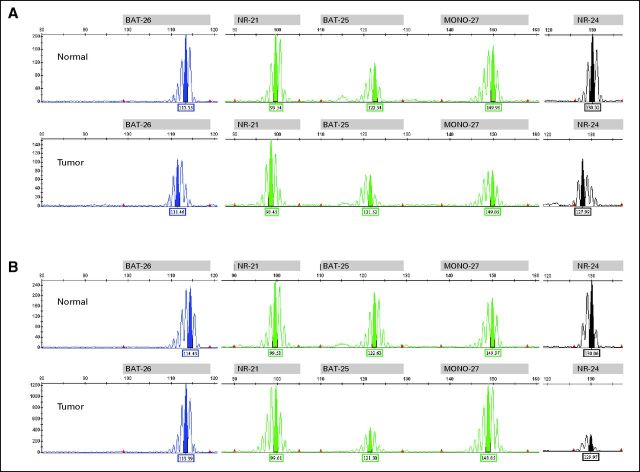
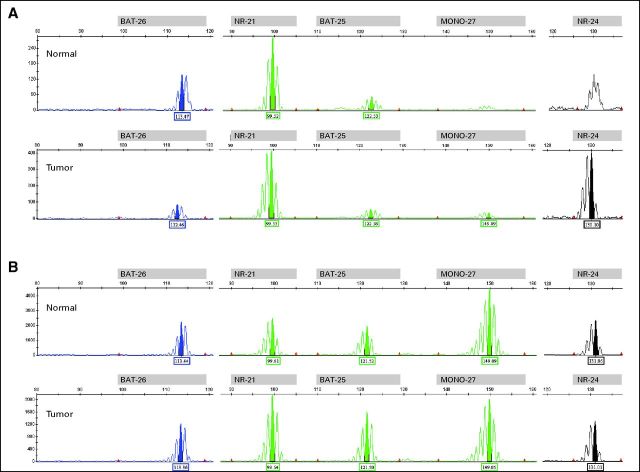
Results: Ninety-four (82.5%) of 114 patients with ACC underwent genetic counseling (group 1). Three individuals (3.2%) had family histories suggestive of LS. All three families were found to have MMR gene mutations. Retrospective review of an additional 135 MMR gene-positive probands identified two with ACC (group 2). Four ACC tumors were available (group 1, 3; group 2, 1). All four tumors were microsatellite stable; three had IHC staining patterns consistent with germline mutation status.
Conclusion: The prevalence of LS among patients with ACC is 3.2%, which is comparable to the prevalence of LS in colorectal and endometrial cancer. Patients with ACC and a personal or family history of LS tumors should be strongly considered for genetic risk assessment. IHC screening of all ACC tumors may be an effective strategy for identifying patients with LS.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Aarnio M, Mecklin JP, Aaltonen LA, et al. Life-time risk of different cancers in hereditary non-polyposis colorectal cancer (HNPCC) syndrome. Int J Cancer. 1995;64:430–433. - PubMed
-
- Aarnio M, Sankila R, Pukkala E, et al. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81:214–218. - PubMed
-
- Järvinen HJ, Aarnio M, Mustonen H, et al. Controlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancer. Gastroenterology. 2000;118:829–834. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
