

Brand-name prescription drug use among Veterans Affairs and Medicare Part D patients with diabetes: a national cohort comparison
- PMID: 23752663
- PMCID: PMC3787067
- DOI: 10.7326/0003-4819-159-2-201307160-00664
Brand-name prescription drug use among Veterans Affairs and Medicare Part D patients with diabetes: a national cohort comparison
Abstract
Background: Medicare Part D and the U.S. Department of Veterans Affairs (VA) use different approaches to manage prescription drug benefits, with implications for spending. Medicare relies on private plans with distinct formularies, whereas the VA administers its own benefit using a national formulary.
Objective: To compare overall and regional rates of brand-name drug use among older adults with diabetes in Medicare and the VA.
Design: Retrospective cohort.
Setting: Medicare and the VA, 2008.
Patients: 1,061,095 Medicare Part D beneficiaries and 510,485 veterans aged 65 years or older with diabetes.
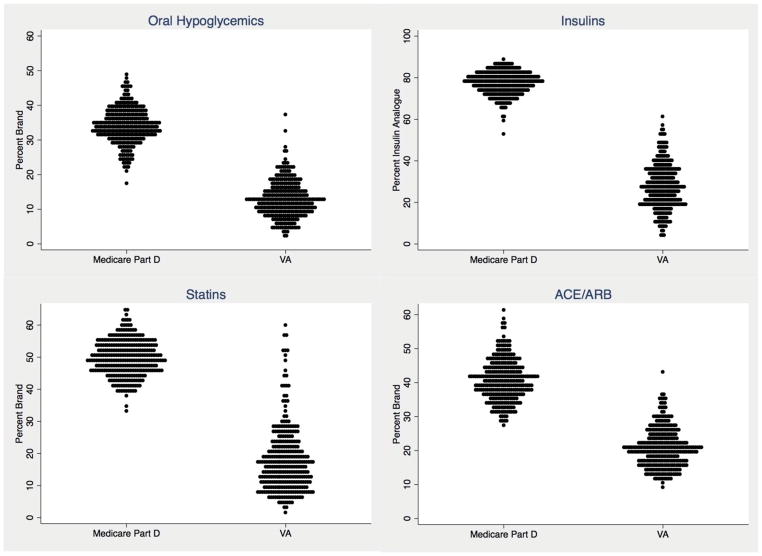
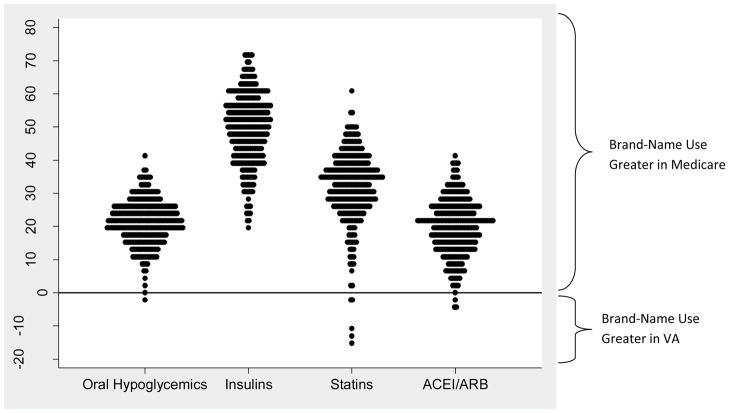
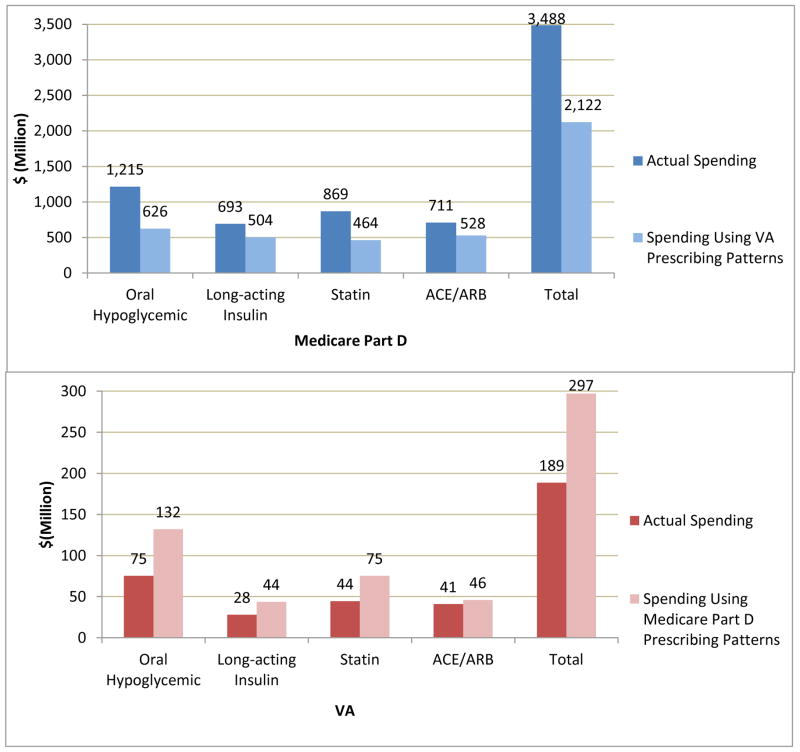
Measurements: Percentage of patients taking oral hypoglycemics, statins, and angiotensin-converting enzyme (ACE) inhibitors or angiotensin-receptor blockers (ARBs) who filled brand-name drug prescriptions and percentage of patients taking long-acting insulins who filled analogue prescriptions. Sociodemographic- and health status-adjusted hospital referral region (HRR) brand-name drug use was compared, and changes in spending were calculated if use of brand-name drugs in 1 system mirrored the other.
Results: Brand-name drug use in Medicare was 2 to 3 times that in the VA: 35.3% versus 12.7% for oral hypoglycemics, 50.7% versus 18.2% for statins, 42.5% versus 20.8% for ACE inhibitors or ARBs, and 75.1% versus 27.0% for insulin analogues. Adjusted HRR-level brand-name statin use ranged (from the 5th to 95th percentiles) from 41.0% to 58.3% in Medicare and 6.2% to 38.2% in the VA. For each drug group, the 95th-percentile HRR in the VA had lower brand-name drug use than the 5th-percentile HRR in Medicare. Medicare spending in this population would have been $1.4 billion less if brand-name drug use matched that of the VA.
Limitation: This analysis cannot fully describe the factors underlying differences in brand-name drug use.
Conclusion: Medicare beneficiaries with diabetes use 2 to 3 times more brand-name drugs than a comparable group within the VA, at substantial excess cost.
Figures
References
-
- Congressional Budget Office. [Accessed April 1, 2012];Effects of Using Generic Drugs on Medicare’s Prescription Drug Spending. 2010 Sep; http://www.cbo.gov/sites/default/files/cbofiles/ftpdocs/118xx/doc11838/0....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous