

Connective tissue ulcers
- PMID: 23756459
- PMCID: PMC3930159
- DOI: 10.1016/j.jtv.2013.04.003
Connective tissue ulcers
Abstract
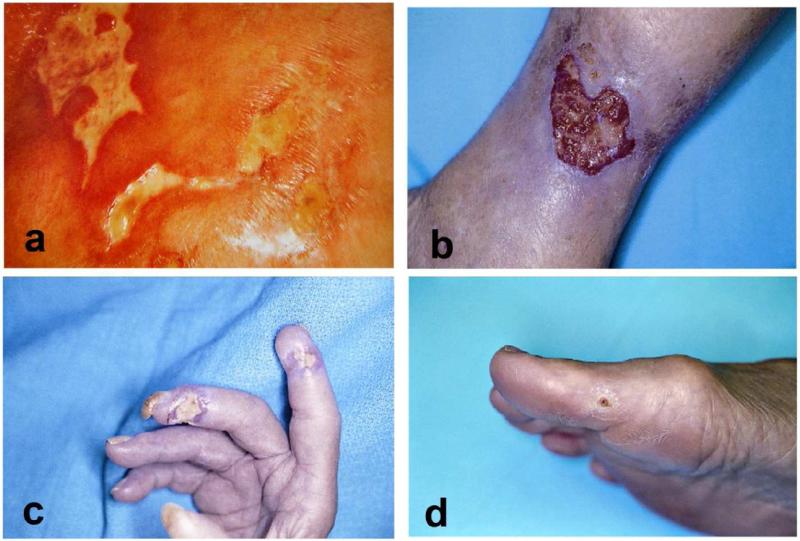
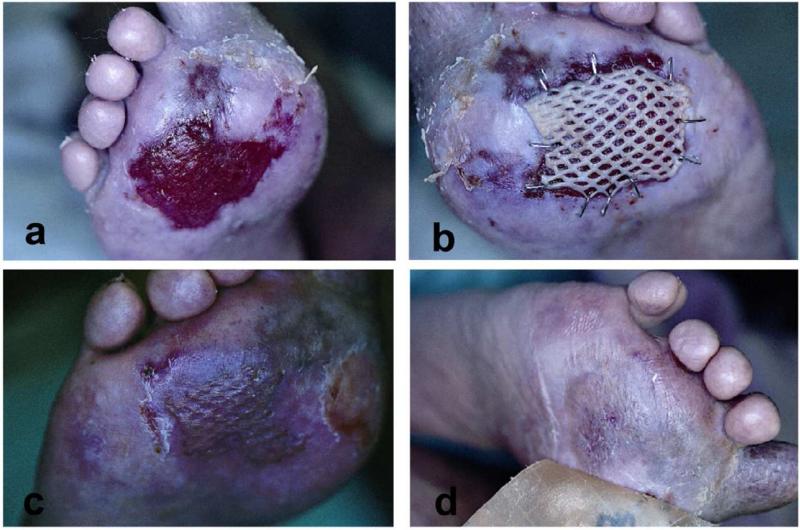
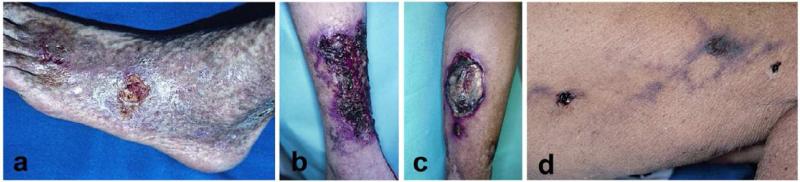
Connective tissue disorders (CTD), which are often also termed collagen vascular diseases, include a number of related inflammatory conditions. Some of these diseases include rheumatoid arthritis, systemic lupus erythematosus, systemic sclerosis (scleroderma), localized scleroderma (morphea variants localized to the skin), Sjogren's syndrome, dermatomyositis, polymyositis, and mixed connective tissue disease. In addition to the systemic manifestations of these diseases, there are a number of cutaneous features that make these conditions recognizable on physical exam. Lower extremity ulcers and digital ulcers are an infrequent but disabling complication of long-standing connective tissue disease. The exact frequency with which these ulcers occur is not known, and the cause of the ulcerations is often multifactorial. Moreover, a challenging component of CTD ulcerations is that there are still no established guidelines for their diagnosis and treatment. The morbidity associated with these ulcerations and their underlying conditions is very substantial. Indeed, these less common but intractable ulcers represent a major medical and economic problem for patients, physicians and nurses, and even well organized multidisciplinary wound healing centers.
Keywords: Connective tissue disease; Connective tissue ulcers; Ulcers; Vasculitis.
Copyright © 2013 Tissue Viability Society. Published by Elsevier Ltd. All rights reserved.
Figures

References
-
- Goslen JB. Autoimmune Ulceration of the leg. Leg Ulcers. 1990;3:92–117. - PubMed
-
- Falanga V, Lindholm C, Carson PA, et al. Text Atlas of Wound Managament (ed 2) Informa Healthcare; London, UK: 2012.
-
- Panuncialman J, Falanga V. Basic approach to inflammatory ulcers. Dermatologic Therapy. 2006;19:365–376. - PubMed
-
- Jorrizo JL, O AJ, Stanely RJ. Superficial Ulcerating Necrobiosis in Rheumatoid Arthritis. A Variant of the Necrobiosis Lipoidica-Rheumatoid Nodule Spectrum? Arch Dermatol. 1982;118 - PubMed
-
- Danning CL, Illei GG, Boumpas DT. Vasculitis associated with primary rheumatologic diseases. Curr opin Rheumatol. 1998;10:58–65. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
