

Impact of dementia on payments for long-term and acute care in an elderly cohort
- PMID: 23756644
- PMCID: PMC3680786
- DOI: 10.1097/MLR.0b013e31828d4d4a
Impact of dementia on payments for long-term and acute care in an elderly cohort
Abstract
Background: Older people with dementia have increased risk of nursing home (NH) use and higher Medicaid payments. Dementia's impact on acute care use and Medicare payments is less well understood.
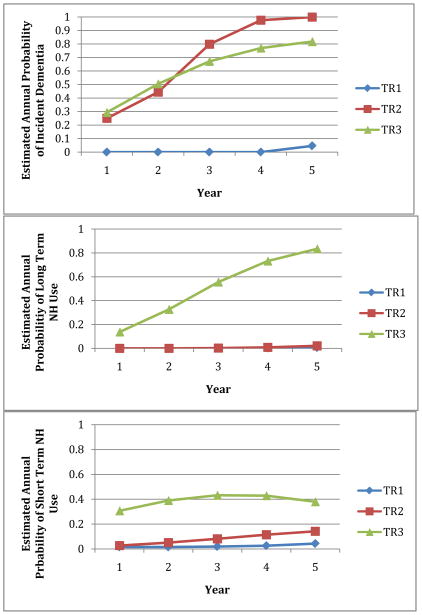
Objectives: Identify trajectories of incident dementia and NH use, and compare Medicare and Medicaid payments for persons having different trajectories.
Research design: Retrospective cohort of older patients who were screened for dementia in 2000-2004 and were tracked for 5 years. Trajectories were identified with latent class growth analysis.
Subjects: A total of 3673 low-income persons aged 65 or older without dementia at baseline.
Measures: Incident dementia diagnosis, comorbid conditions, dual eligibility, acute and long-term care use and payments based on Medicare and Medicaid claims, medical record systems, and administrative data.
Results: Three trajectories were identified based on dementia incidence and short-term and long-term NH use: (1) high incidence of dementia with heavy NH use (5% of the cohort) averaging $56,111/year ($36,361 Medicare, $19,749 Medicaid); (2) high incidence of dementia with little or no NH use (16% of the cohort) averaging $16,206/year ($14,644 Medicare, $1562 Medicaid); and (3) low incidence of dementia and little or no NH use (79% of the cohort) averaging $8475/year ($7558 Medicare, $917 Medicaid).
Conclusions: Dementia and its interaction with NH utilization are major drivers of publicly financed acute and long-term care payments. Medical providers in Accountable Care Organizations and other health care reform efforts must effectively manage dementia care across the care continuum if they are to be financially viable.
Figures
References
-
- HealthCare.gov. [Accessed April 20, 2012];Compilation of the Patient Protection and Affordable Care Act. 2010. 2012 Available at: http://www.healthcare.gov/law/full/index.html.
-
- Luppa M, Luck T, Weyerer S, et al. Prediction of institutionalization in the elderly. A systematic review. Age Ageing. 2010;39:31–38. - PubMed
-
- Welch HG, Walsh JS, Larson EB. The cost of institutional care in Alzheimer’s disease: nursing home and hospital use in a prospective cohort. J Am Geriatr Soc. 1992;40:221–224. - PubMed
-
- Smith GE, O’Brien PC, Ivnik RJ, et al. Prospective analysis of risk factors for nursing home placement of dementia patients. Neurology. 2001;57:1467–1473. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
