

Clinical ascertainment of health outcomes among adults treated for childhood cancer
- PMID: 23757085
- PMCID: PMC3771083
- DOI: 10.1001/jama.2013.6296
Clinical ascertainment of health outcomes among adults treated for childhood cancer
Erratum in
- JAMA. 2013 Jul 3;310(1):99
Abstract
Importance: Adult survivors of childhood cancer are known to be at risk for treatment-related adverse health outcomes. A large population of survivors has not been evaluated using a comprehensive systematic clinical assessment to determine the prevalence of chronic health conditions.
Objective: To determine the prevalence of adverse health outcomes and the proportion associated with treatment-related exposures in a large cohort of adult survivors of childhood cancer.
Design, setting, and participants: Presence of health outcomes was ascertained using systematic exposure-based medical assessments among 1713 adult (median age, 32 [range, 18-60] years) survivors of childhood cancer (median time from diagnosis, 25 [range, 10-47] years) enrolled in the St Jude Lifetime Cohort Study since October 1, 2007, and undergoing follow-up through October 31, 2012.
Main outcomes and measures: Age-specific cumulative prevalence of adverse outcomes by organ system.
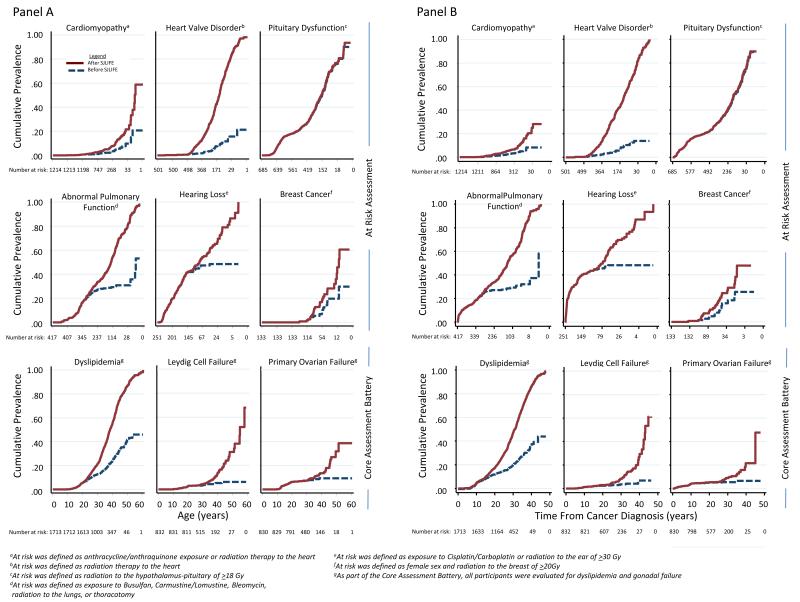
Results: Using clinical criteria, the crude prevalence of adverse health outcomes was highest for pulmonary (abnormal pulmonary function, 65.2% [95% CI, 60.4%-69.8%]), auditory (hearing loss, 62.1% [95% CI, 55.8%-68.2%]), endocrine or reproductive (any endocrine condition, such as hypothalamic-pituitary axis disorders and male germ cell dysfunction, 62.0% [95% CI, 59.5%-64.6%]), cardiac (any cardiac condition, such as heart valve disorders, 56.4% [95% CI, 53.5%-59.2%]), and neurocognitive (neurocognitive impairment, 48.0% [95% CI, 44.9%-51.0%]) function, whereas abnormalities involving hepatic (liver dysfunction, 13.0% [95% CI, 10.8%-15.3%]), skeletal (osteoporosis, 9.6% [95% CI, 8.0%-11.5%]), renal (kidney dysfunction, 5.0% [95% CI, 4.0%-6.3%]), and hematopoietic (abnormal blood cell counts, 3.0% [95% CI, 2.1%-3.9%]) function were less common. Among survivors at risk for adverse outcomes following specific cancer treatment modalities, the estimated cumulative prevalence at age 50 years was 21.6% (95% CI, 19.3%-23.9%) for cardiomyopathy, 83.5% (95% CI, 80.2%-86.8%) for heart valve disorder, 81.3% (95% CI, 77.6%-85.0%) for pulmonary dysfunction, 76.8% (95% CI, 73.6%-80.0%) for pituitary dysfunction, 86.5% (95% CI, 82.3%-90.7%) for hearing loss, 31.9% (95% CI, 28.0%-35.8%) for primary ovarian failure, 31.1% (95% CI, 27.3%-34.9%) for Leydig cell failure, and 40.9% (95% CI, 32.0%-49.8%) for breast cancer. At age 45 years, the estimated cumulative prevalence of any chronic health condition was 95.5% (95% CI, 94.8%-98.6%) and 80.5% (95% CI, 73.0%-86.6%) for a serious/disabling or life-threatening chronic condition.
Conclusions and relevance: Among adult survivors of childhood cancer, the prevalence of adverse health outcomes was high, and a systematic risk-based medical assessment identified a substantial number of previously undiagnosed problems that are more prevalent in an older population. These findings underscore the importance of ongoing health monitoring for adults who survive childhood cancer.
Figures
References
-
- Geenen MM, Cardous-Ubbink MC, Kremer LC, et al. Medical assessment of adverse health outcomes in long-term survivors of childhood cancer. JAMA. 2007;297(24):2705–2715. - PubMed
-
- Oeffinger KC, Mertens AC, Sklar CA, et al. Chronic health conditions in adult survivors of childhood cancer. N Engl J Med. 2006;355(15):1572–1582. - PubMed
-
- Rebholz CE, Reulen RC, Toogood AA, et al. Health care use of long-term survivors of childhood cancer: the British Childhood Cancer Survivor Study. J Clin Oncol. 2011;29(31):4181–4188. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
