

Role of relaxin-2 in human primary osteosarcoma
- PMID: 23758748
- PMCID: PMC3698148
- DOI: 10.1186/1475-2867-13-59
Role of relaxin-2 in human primary osteosarcoma
Abstract
Background: The aim of this study was to clarify the clinicopathological outcome of serum relaxin-2 and tissues relaxin-2 expression levels in human primary osteosarcoma (OS), and to explore the roles of relaxin-2 inhibition and determine its possibility as a therapeutic target in human osteosarcoma.
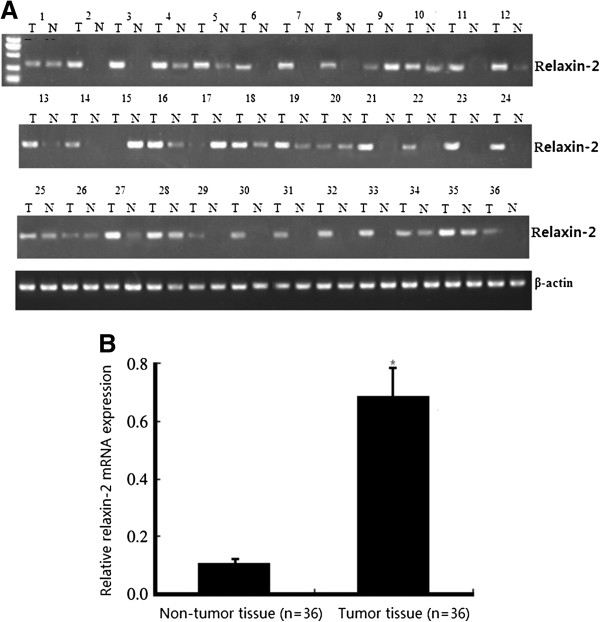
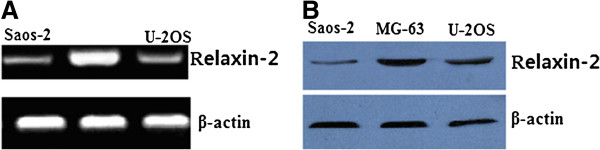
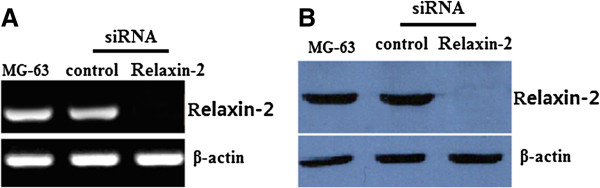
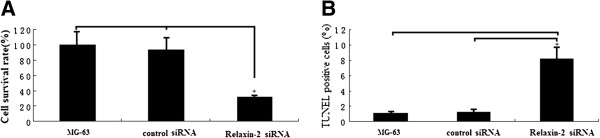
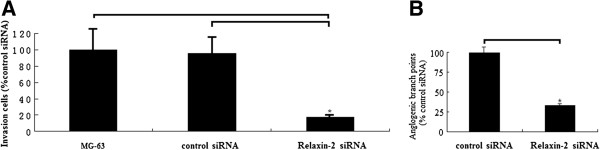
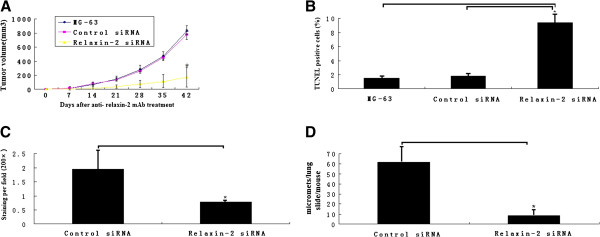
Methods: Real-time quantitative RT-PCR assay was performed to detect the expression of relaxin-2 mRNA in 36 cases of human osteosarcoma tissue samples. Serum relaxin-2 levels was measured in ELISA-based method in the 36 cases of osteosarcoma and 50 cases of controls. MTT and TUNEL assay was used to detect cell proliferation and apoptosis after relaxin-2 knockdown with siRNA transfection for 48 hs in vitro. Matrigel invasion and angiogenesis formation assay was used to detect cell metastasis and angiogenesis with HMEC-1 endothelial cells after relaxin-2 knockdown with siRNA transfection for 48 hs in vitro. The effects of relaxin-2 knockdown with anti- relaxin-2 mAb treatment on growth, apoptosis angiogenesis formation and lung metastasis in vivo was analyzed.
Results: The results showed the levels of relaxin-2 mRNA expression in osteosarcoma tissue samples were significantly higher than those in the corresponding non-tumor tissue samples (P < 0.01), and the serum relaxin-2 levels were significantly higher in OS patients than in healthy controls (P < 0.01). The incidence of advanced stage cancer and hematogenous metastasis cancer in the high relaxin-2 mRNA expression group and high serum relaxin-2 levels groups was significantly higher than that in the low relaxin-2 expression group and low serum relaxin-2 levels groups, respectively. Knockdown of relaxin-2 by siRNA transfection in vitro inhibited proliferation, invasion and angiogenesis in vitro in MG-63 OS cells. In vivo, knockdown of relaxin-2 with anti- relaxin-2 mAb treatment inhibited tumor growth by 62% (P < 0.01) and the formation of lung metastases was inhibited by 72.4% (P < 0.01). Microvascular density was reduced more than 60% due to anti- relaxin-2 mAb treatment (P < 0.01).
Conclusions: Our study suggests that overexpression of relaxin-2 is critical for the metastasis of human osteosarcoma. Detection of relaxin-2 mRNA expression or serum relaxin-2 levels may provide the first biological prognostic marker for OS. Furthermore, relaxin-2 is the potential molecular target for osteosarcoma therapy.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
