

Danger control programs cause tissue injury and remodeling
- PMID: 23759985
- PMCID: PMC3709734
- DOI: 10.3390/ijms140611319
Danger control programs cause tissue injury and remodeling
Abstract
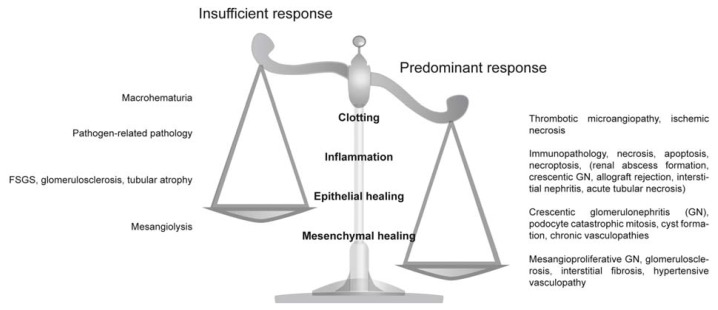
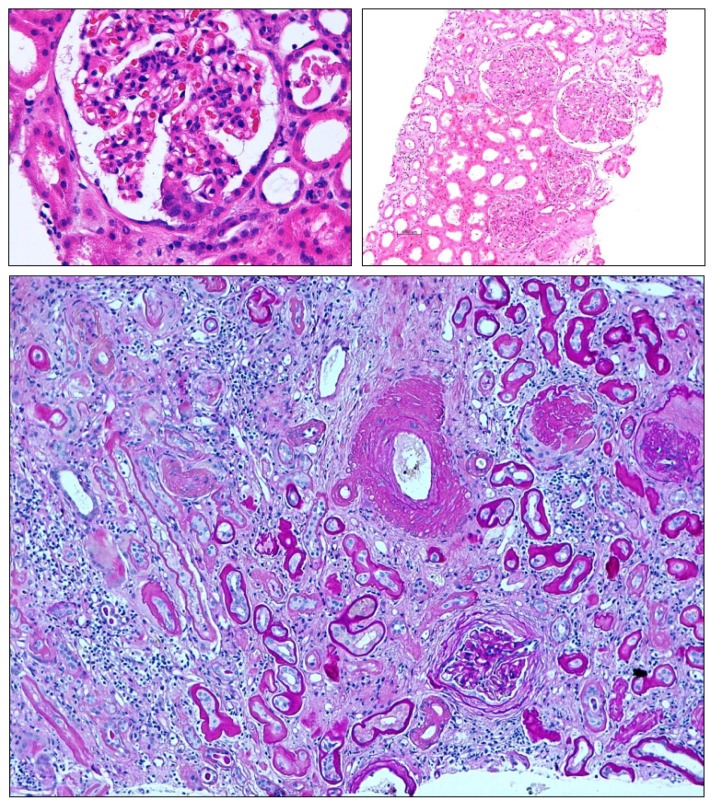
Are there common pathways underlying the broad spectrum of tissue pathologies that develop upon injuries and from subsequent tissue remodeling? Here, we explain the pathophysiological impact of a set of evolutionary conserved danger control programs for tissue pathology. These programs date back to the survival benefits of the first multicellular organisms upon traumatic injuries by launching a series of danger control responses, i.e., 1. Haemostasis, or clotting to control bleeding; 2. Host defense, to control pathogen entry and spreading; 3. Re-epithelialisation, to recover barrier functions; and 4. Mesenchymal, to repair to regain tissue stability. Taking kidney pathology as an example, we discuss how clotting, inflammation, epithelial healing, and fibrosis/sclerosis determine the spectrum of kidney pathology, especially when they are insufficiently activated or present in an overshooting and deregulated manner. Understanding the evolutionary benefits of these response programs may refine the search for novel therapeutic targets to limit organ dysfunction in acute injuries and in progressive chronic tissue remodeling.
Figures
References
-
- Schilmiller A.L., Howe G.A. Systemic signaling in the wound response. Curr. Opin. Plant Biol. 2005;8:369–377. - PubMed
-
- Gurtner G.C., Werner S., Barrandon Y., Longaker M.T. Wound repair and regeneration. Nature. 2008;453:314–321. - PubMed
-
- Singer A.J., Clark R.A. Cutaneous wound healing. N. Engl. J. Med. 1999;341:738–746. - PubMed
-
- Clark R.A. Cutaneous tissue repair: Basic biologic considerations. I. J. Am. Acad. Dermatol. 1985;13:701–725. - PubMed
-
- Martin P. Wound healing—Aiming for perfect skin regeneration. Science. 1997;276:75–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
