

Acute respiratory distress syndrome after spontaneous intracerebral hemorrhage*
- PMID: 23760151
- PMCID: PMC3752686
- DOI: 10.1097/CCM.0b013e31828a3f4d
Acute respiratory distress syndrome after spontaneous intracerebral hemorrhage*
Abstract
Objectives: Acute respiratory distress syndrome develops commonly in critically ill patients in response to an injurious stimulus. The prevalence and risk factors for development of acute respiratory distress syndrome after spontaneous intracerebral hemorrhage have not been reported. We sought to determine the prevalence of acute respiratory distress syndrome after intracerebral hemorrhage, characterize risk factors for its development, and assess its impact on patient outcomes.
Design: Retrospective cohort study at two academic centers.
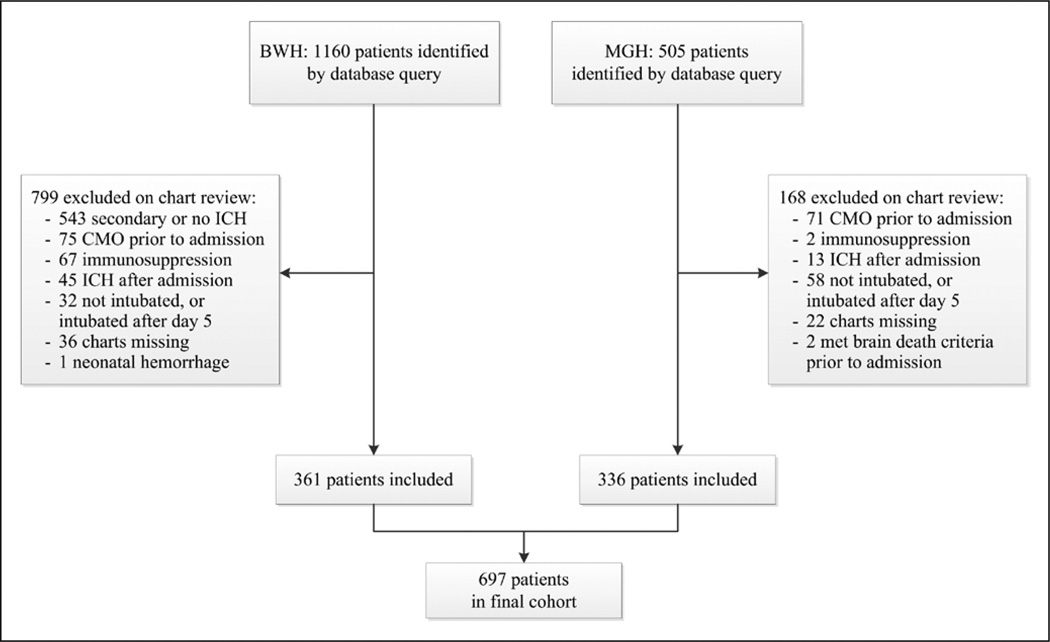
Patients: We included consecutive patients presenting from June 1, 2000, to November 1, 2010, with intracerebral hemorrhage requiring mechanical ventilation. We excluded patients with age less than 18 years, intracerebral hemorrhage secondary to trauma, tumor, ischemic stroke, or structural lesion; if they required intubation only during surgery; if they were admitted for comfort measures; or for a history of immunodeficiency.
Interventions: None.
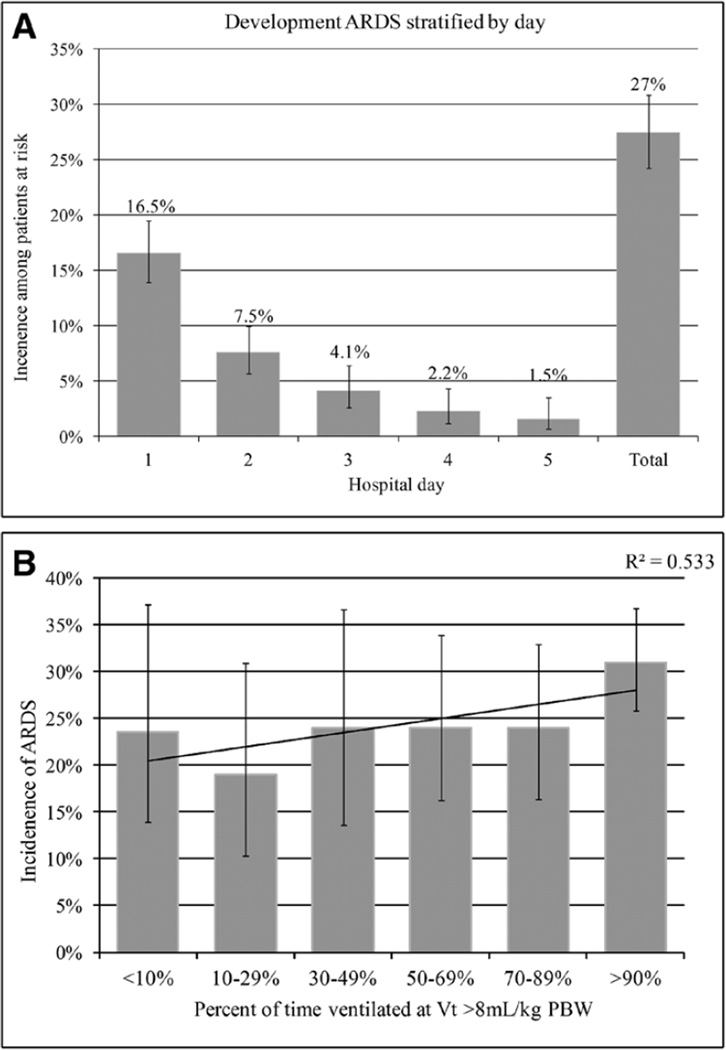
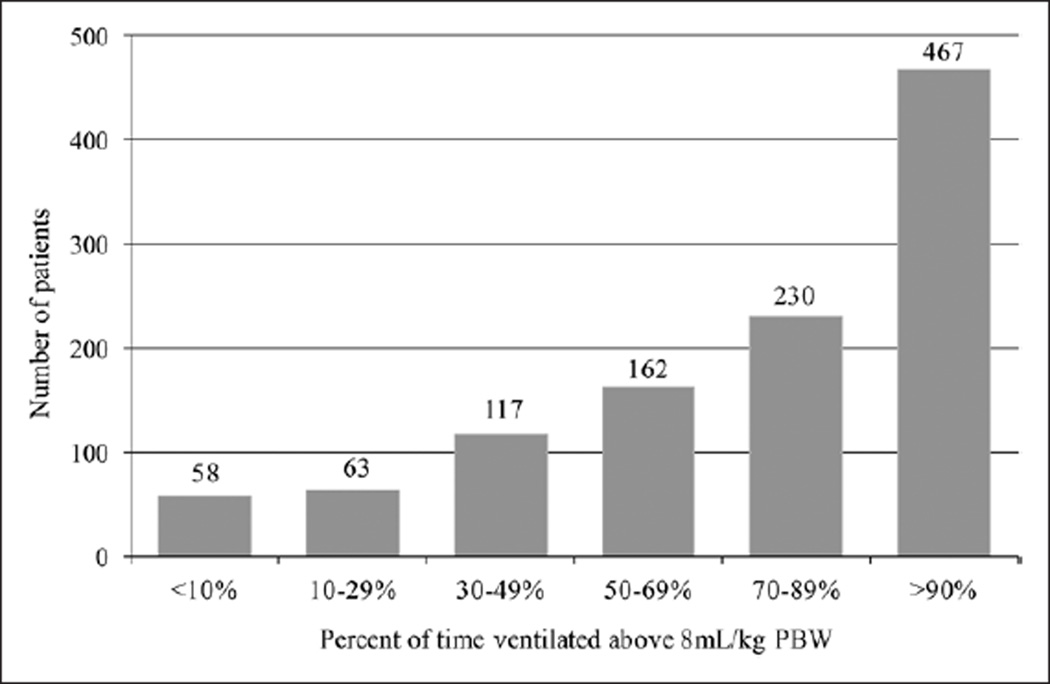
Measurements and main results: Data were collected both prospectively as part of an ongoing cohort study and by retrospective chart review. Of 1,665 patients identified by database query, 697 met inclusion criteria. The prevalence of acute respiratory distress syndrome was 27%. In unadjusted analysis, high tidal volume ventilation was associated with an increased risk of acute respiratory distress syndrome (hazard ratio, 1.79 [95% CI, 1.13-2.83]), as were male sex, RBC and plasma transfusion, higher fluid balance, obesity, hypoxemia, acidosis, tobacco use, emergent hematoma evacuation, and vasopressor dependence. In multivariable modeling, high tidal volume ventilation was the strongest risk factor for acute respiratory distress syndrome development (hazard ratio, 1.74 [95% CI, 1.08-2.81]) and for inhospital mortality (hazard ratio, 2.52 [95% CI, 1.46-4.34]).
Conclusions: Development of acute respiratory distress syndrome is common after intubation for intracerebral hemorrhage. Modifiable risk factors, including high tidal volume ventilation, are associated with its development and in-patient mortality.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
-
Acute respiratory distress syndrome: rather a (vague) concept than a (clear) definition*.Crit Care Med. 2013 Aug;41(8):2055-6. doi: 10.1097/CCM.0b013e31828fd91e. Crit Care Med. 2013. PMID: 23863248 No abstract available.
Similar articles
-
Clinician Recognition of the Acute Respiratory Distress Syndrome: Risk Factors for Under-Recognition and Trends Over Time.Crit Care Med. 2020 Jun;48(6):830-837. doi: 10.1097/CCM.0000000000004328. Crit Care Med. 2020. PMID: 32317598 Free PMC article.
-
Acute respiratory distress syndrome: rather a (vague) concept than a (clear) definition*.Crit Care Med. 2013 Aug;41(8):2055-6. doi: 10.1097/CCM.0b013e31828fd91e. Crit Care Med. 2013. PMID: 23863248 No abstract available.
-
Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation.Crit Care Med. 2004 Sep;32(9):1817-24. doi: 10.1097/01.ccm.0000133019.52531.30. Crit Care Med. 2004. PMID: 15343007
-
Ventilator strategies for posttraumatic acute respiratory distress syndrome: airway pressure release ventilation and the role of spontaneous breathing in critically ill patients.Curr Opin Crit Care. 2004 Dec;10(6):549-57. doi: 10.1097/01.ccx.0000145473.01597.13. Curr Opin Crit Care. 2004. PMID: 15616399 Review.
-
Controversies when using mechanical ventilation in obese patients with and without acute distress respiratory syndrome.Expert Rev Respir Med. 2019 May;13(5):471-479. doi: 10.1080/17476348.2019.1599285. Epub 2019 Apr 5. Expert Rev Respir Med. 2019. PMID: 30919705 Review.
Cited by
-
Respiratory Parameters as Predictors of Balance and Gait Ability in Patients with Stroke at Discharge.Int J Environ Res Public Health. 2023 Nov 22;20(23):7098. doi: 10.3390/ijerph20237098. Int J Environ Res Public Health. 2023. PMID: 38063528 Free PMC article.
-
Mechanical ventilation in patients with acute brain injury: a systematic review with meta-analysis.Crit Care. 2023 Jun 6;27(1):221. doi: 10.1186/s13054-023-04509-3. Crit Care. 2023. PMID: 37280579 Free PMC article.
-
Brain-Lung Crosstalk: Management of Concomitant Severe Acute Brain Injury and Acute Respiratory Distress Syndrome.Curr Treat Options Neurol. 2022;24(9):383-408. doi: 10.1007/s11940-022-00726-3. Epub 2022 Aug 10. Curr Treat Options Neurol. 2022. PMID: 35965956 Free PMC article. Review.
-
Letter: Hemorrhagic Conditions Affecting the Central Nervous System in COVID-19 Patients.Neurosurgery. 2020 Sep 1;87(3):E394-E396. doi: 10.1093/neuros/nyaa253. Neurosurgery. 2020. PMID: 32490520 Free PMC article. No abstract available.
-
Emerging concepts in ventilation-induced lung injury.F1000Res. 2020 Mar 31;9:F1000 Faculty Rev-222. doi: 10.12688/f1000research.20576.1. eCollection 2020. F1000Res. 2020. PMID: 32269759 Free PMC article. Review.
References
-
- Shanahan WT. Acute pulmonary edema as a complication of epileptic seizures. NY Med J. 1908;54:54–56.
-
- Wu S, Fang CX, Kim J, et al. Enhanced pulmonary inflammation following experimental intracerebral hemorrhage. Exp Neurol. 2006;200:245–249. - PubMed
-
- Ott L, McClain CJ, Gillespie M, et al. Cytokines and metabolic dysfunction after severe head injury. J Neurotrauma. 1994;11:447–472. - PubMed
-
- Mascia L, Zavala E, Bosma K, et al. Brain IT group: High tidal volume is associated with the development of acute lung injury after severe brain injury An international observational study. Crit Care Med. 2007;35:1815–1820. - PubMed
-
- Dziedzic T, Bartus S, Klimkowicz A, et al. Intracerebral hemorrhage triggers interleukin-6 and interleukin-10 release in blood. Stroke. 2002;33:2334–2335. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
