

External validity of the Society of Thoracic Surgeons risk stratification tool for deep sternal wound infection after cardiac surgery in a UK population
- PMID: 23760358
- PMCID: PMC3745138
- DOI: 10.1093/icvts/ivt222
External validity of the Society of Thoracic Surgeons risk stratification tool for deep sternal wound infection after cardiac surgery in a UK population
Abstract
Objectives: Deep sternal wound infection (DSWI) is a devastating complication of cardiac surgery, with a historical incidence of 0.4-5%. Predicting which patients are at higher risk of infection may help instituting various preventive measures. Risk calculations for mortality have been used as surrogates to estimate the risk of deep sternal wound infection, with limited success. The Society of Thoracic Surgeons (STS) 2008 Risk Calculator modelled the risk of DSWI for cardiac surgical patients, but it has not been validated since its publication. We sought to assess the external validity of the STS-estimated risk of DSWI in a United Kingdom (UK) population.
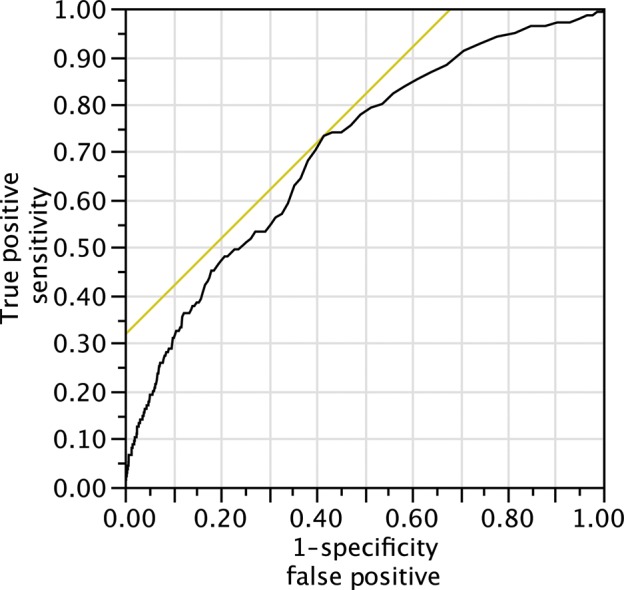
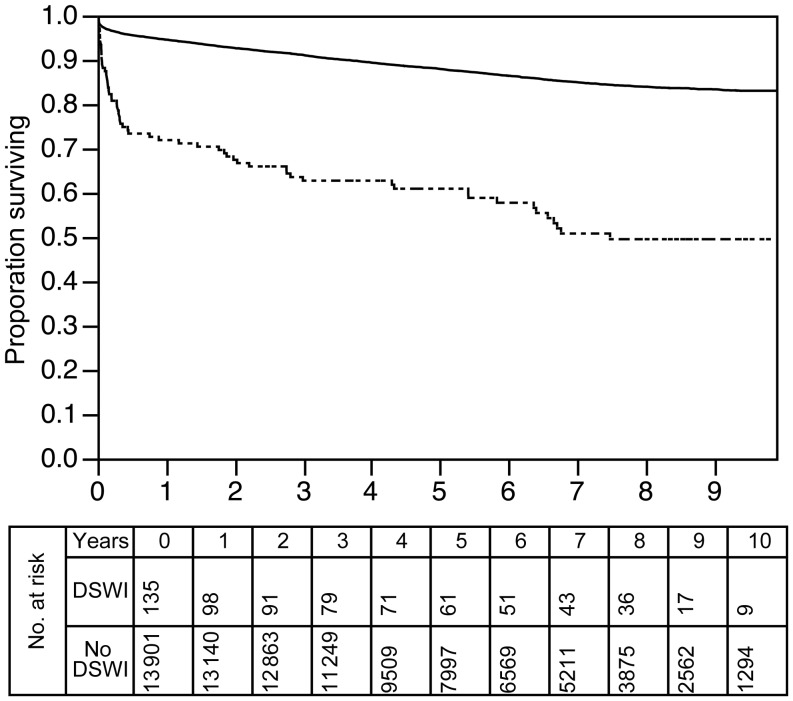
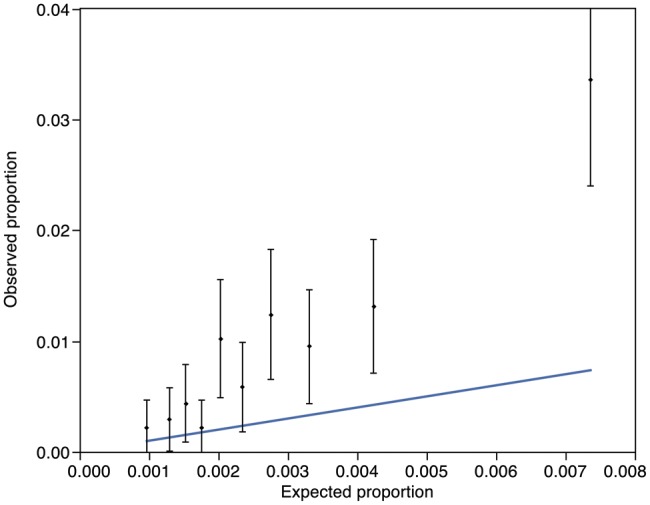
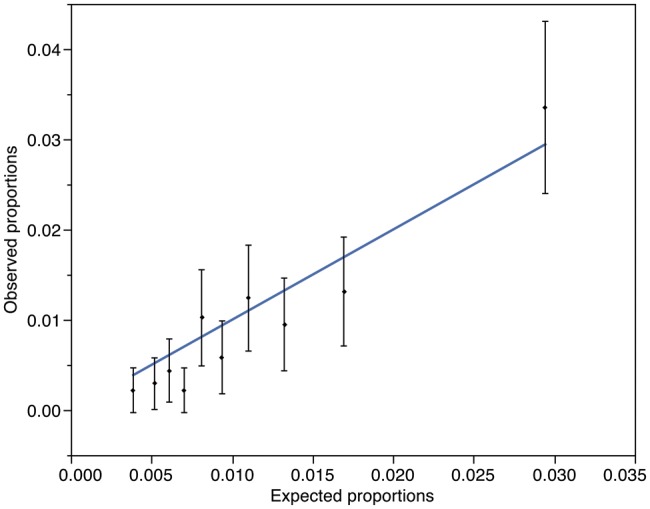
Methods: Using our prospectively captured database, we retrospectively calculated the risk of DSWI for 14 036 patients undergoing valve, coronary artery bypass grafts or combined procedures between February 2001 and March 2010. DSWI was identified according to the Centre for Disease Control and Prevention definition. The receiver operator characteristic (ROC) curve was employed to test the performance of the model using the area under the ROC curve (AUROC). The calibration of the model was interrogated using the Hosmer-Lemeshow test for Goodness of Fit.
Results: A total of 135 (0.95%) patients developed DSWI. Although there was a statistically significant difference in the calculated risk of patients who contracted DSWI (0.44% ± 0.01) vs those who did not (0.28% ± 0.00, P < 0.0001), the AUROC of 0.699 (95% confidence interval: 0.6522-0.7414) denoted a modest discriminatory power, with the Hosmer-Lemeshow Goodness of Fit statistic (P < 0.001) suggesting poor calibration. A risk-adjusted modifier improved the calibration (P = 0.08).
Conclusions: The STS risk calculator lacks adequate discriminatory power for estimating the isolated risk of developing deep sternal wound infection in a UK population. The discrimination is similar to the tool's validation c-statistic and may have a place in an integrated calculator.
Keywords: Complications; Infection; Risk analysis/modelling; Statistics; Sternum.
Figures
References
-
- Ottino G, De Paulis R, Pansini S, Rocca G, Tallone MV, Comoglio C, et al. Major sternal wound infection after open-heart surgery: a multivariate analysis of risk factors in 2,579 consecutive operative procedures. Ann Thorac Surg. 1987;44:173–9. doi:10.1016/S0003-4975(10)62035-8. - DOI - PubMed
-
- Braxton JH, Marrin CAS, McGrath PD, Morton JR, Norotsky M, Charlesworth DC, et al. 10-year follow-up of patients with and without mediastinitis. Semin Thorac Cardiovasc Surg. 2004;16:70–6. doi:10.1053/j.semtcvs.2004.01.006. - DOI - PubMed
-
- He G-W, Ryan WH, Acuff TE, Bowman RT, Douthit MB, Yang C-Q, et al. Risk factors for operative mortality and sternal wound infection in bilateral internal mammary artery grafting. J Thorac Cardiovasc Surg. 1994;107:196–202. - PubMed
-
- Kouchoukos NT, Wareing TH, Murphy SF, Pelate C, Marshall WG. Risks of bilateral internal mammary artery bypass grafting. Ann Thorac Surg. 1990;49:210–9. doi:10.1016/0003-4975(90)90140-2. - DOI - PubMed
-
- The Parisian Mediastinitis Study Group. Risk factors for deep sternal wound infection after sternotomy: a prospective, multicenter study. J Thorac Cardiovasc Surg. 1996;111:1200–7. doi:10.1016/S0022-5223(96)70222-2. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
