

Prospective study of restless legs syndrome and mortality among men
- PMID: 23761622
- PMCID: PMC3770202
- DOI: 10.1212/WNL.0b013e318297eee0
Prospective study of restless legs syndrome and mortality among men
Abstract
Objective: To prospectively examine whether men with restless legs syndrome (RLS) had an increased risk of mortality.
Method: This was a prospective cohort study of 18,425 US men free of diabetes, arthritis, and renal failure in the Health Professionals Follow-up Study (HPFS). In 2002, RLS was assessed using a set of standardized questions. Deaths were identified from state vital statistics records, the National Death Index, family reports, and the postal system.
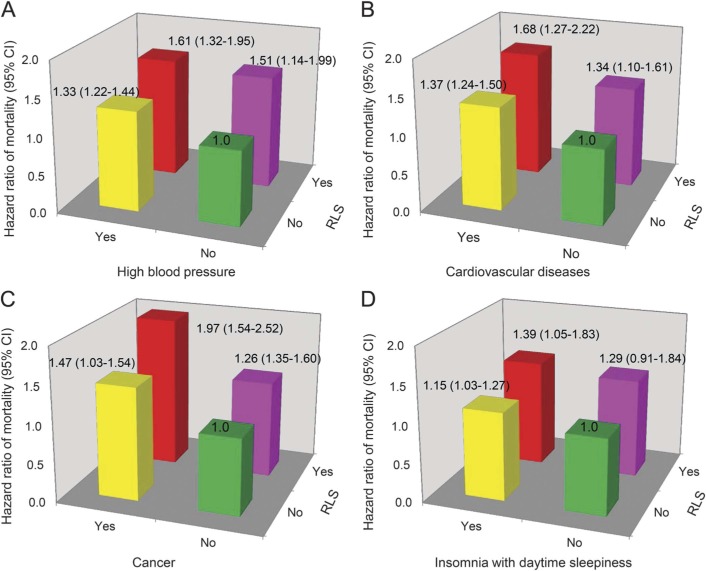
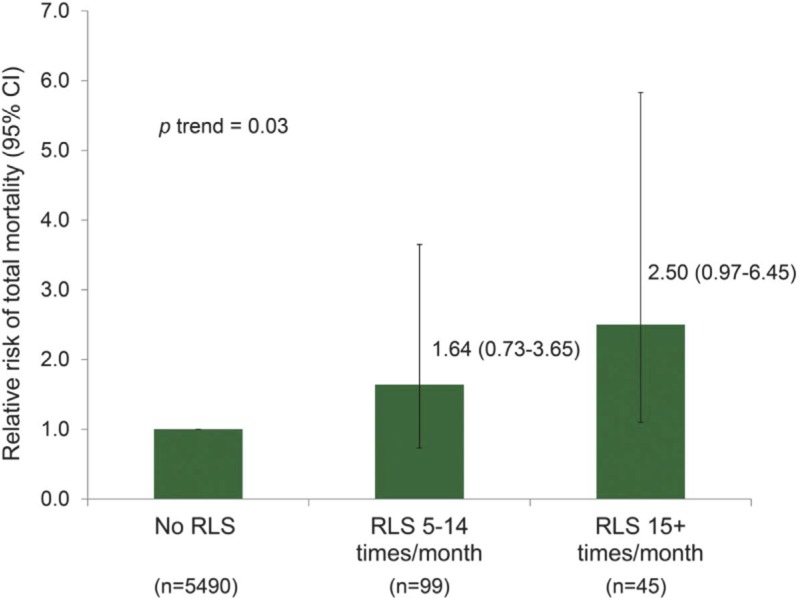
Results: During 8 years of follow-up (2002-2010), we documented 2,765 deaths. In an age-adjusted model, RLS was associated with a 39% increased risk of mortality (hazard ratio [HR] = 1.39; 95% confidence interval [CI] 1.19-1.62; p < 0.0001). The association between RLS and mortality was slightly attenuated after further adjustment for body mass index, lifestyle factors, chronic conditions, sleep duration, and other sleep-related disorders (adjusted HR = 1.30; 95% CI 1.11-1.52; p = 0.003). When we further excluded those with major chronic conditions (e.g., cancer, high blood pressure, cardiovascular disease, and other comorbidities), the adjusted HR was 1.92 (95% CI 1.03-3.56; p = 0.04). The interactions between RLS and other risk factors (older age, overweight, short sleep duration, smoking, low physical activity, and unhealthy diet) in relation to total mortality risk were not significant (p for interaction >0.2 for all).
Conclusion: We observed that men with RLS had a higher overall mortality and this association was independent of known risk factors. The increased mortality in RLS was more frequently associated with respiratory disease, endocrine disease, nutritional/metabolic disease, and immunologic disorders. Future research exploring the pathophysiologic relationship between these disorders and RLS is warranted.
Figures
References
-
- Hening WA, Allen RP, Chaudhuri KR, et al. Clinical significance of RLS. Mov Disord 2007;22:S395–S400 - PubMed
-
- Ekbom K. Restless legs syndrome. Neurology 1960;10:868–873 - PubMed
-
- Restless Legs Syndrome Foundation. Available at: http://www.rls.org/Document.Doc?id=2127. Accessed January 27, 2012
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical