

Reduced incidence of cardiac arrhythmias in walkers and runners
- PMID: 23762337
- PMCID: PMC3676466
- DOI: 10.1371/journal.pone.0065302
Reduced incidence of cardiac arrhythmias in walkers and runners
Abstract
Purpose: Walking is purported to reduce the risk of atrial fibrillation by 48%, whereas jogging is purported to increase its risk by 53%, suggesting a strong anti-arrhythmic benefit of walking over running. The purpose of these analyses is to compare incident self-reported physician-diagnosed cardiac arrhythmia to baseline energy expenditure (metabolic equivalent hours per day, METhr/d) from walking, running and other exercise.
Methods: Proportional hazards analysis of 14,734 walkers and 32,073 runners.
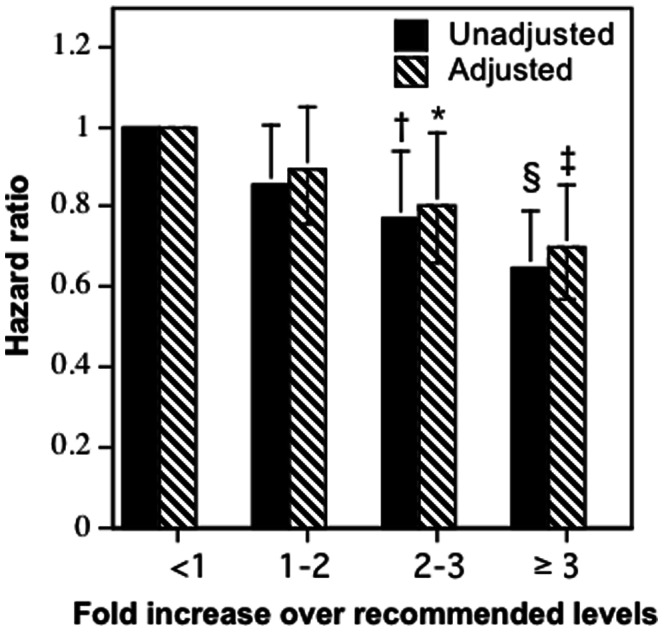
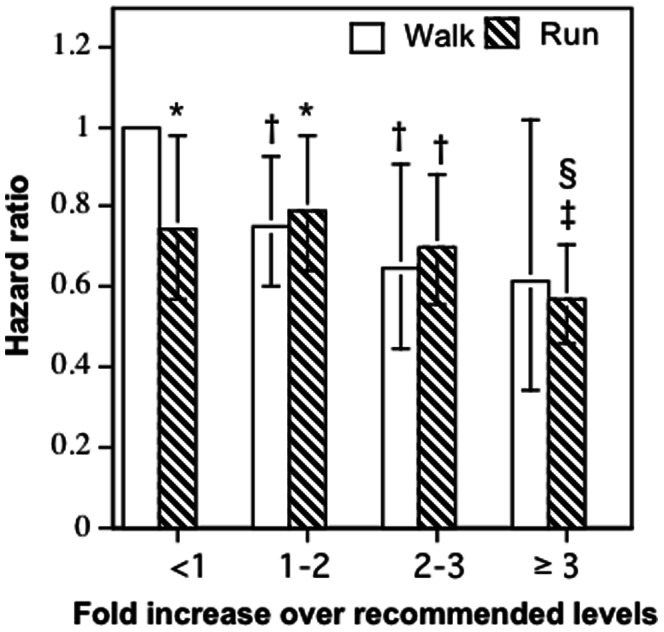
Results: There were 1,060 incident cardiac arrhythmias (412 walkers, 648 runners) during 6.2 years of follow-up. The risk for incident cardiac arrhythmias declined 4.4% per baseline METhr/d walked by the walkers, or running in the runners (P = 0.0001). Specifically, the risk declined 14.2% (hazard ratio: 0.858) for 1.8 to 3.6 METhr/d, 26.5% for 3.6 to 5.4 METhr/d, and 31.7% for ≥5.4 METhr/d, relative to <1.8 METhr/d. The risk reduction per METhr/d was significantly greater for walking than running (P<0.01), but only because walkers were at 34% greater risk than runners who fell below contemporary physical activity guideline recommendations; otherwise the walkers and runners had similar risks for cardiac arrhythmias. Cardiac arrhythmias were unrelated to walking and running intensity, and unrelated to marathon participation and performance.
Conclusions: The risk for cardiac arrhythmias was similar in walkers and runners who expended comparable METhr/d during structured exercise. We found no significant risk increase for self-reported cardiac arrhythmias associated with running distance, exercise intensity, or marathon participation. Rhythm abnormalities were based on self-report, precluding definitive categorization of the nature of the rhythm disturbance. However, even if the runners' arrhythmias include sinus bradycardia due to running itself, there was no increase in arrhythmias with greater running distance.
Conflict of interest statement
Figures
References
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D (1998) Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 82: 2N–9N. - PubMed
-
- Rosamond W, Flegal K, Friday G, Furie K, Go A, et al. (2007) Heart disease and stroke statistics–2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 115: e69–e171. - PubMed
-
- Wolf PA, Mitchell JB, Baker CS, Kannel WB, D’Agostino RB (1998) Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. 158: 229–34. - PubMed
-
- Psaty BM, Manolio TA, Kuller LH, Kronmal RA, Cushman M, et al. (1997) Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 96: 2455–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
