

Time to treatment and patient outcomes among TB suspects screened by a single point-of-care xpert MTB/RIF at a primary care clinic in Johannesburg, South Africa
- PMID: 23762367
- PMCID: PMC3675091
- DOI: 10.1371/journal.pone.0065421
Time to treatment and patient outcomes among TB suspects screened by a single point-of-care xpert MTB/RIF at a primary care clinic in Johannesburg, South Africa
Abstract
Introduction: In December 2010, the World Health Organization recommended a single Xpert MTB/RIF assay as the initial diagnostic in people suspected of HIV-associated or drug resistant tuberculosis. Few data are available on the impact of this recommendation on patient outcomes. We describe the diagnostic follow-up, clinical characteristics and outcomes of a cohort of tuberculosis suspects screened using a single point-of-care Xpert.
Methods: Consecutive tuberculosis suspects at a primary care clinic in Johannesburg, South Africa were assessed for tuberculosis using point-of-care Xpert. Sputum smear microscopy and liquid culture were performed as reference standards. Xpert-negatives were evaluated clinically, and further assessed at the discretion of clinicians. Participants were followed for six months.
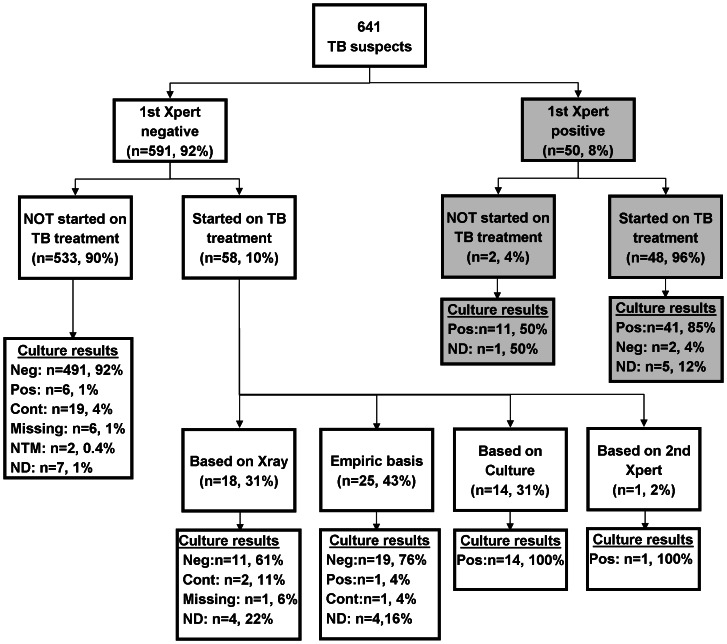
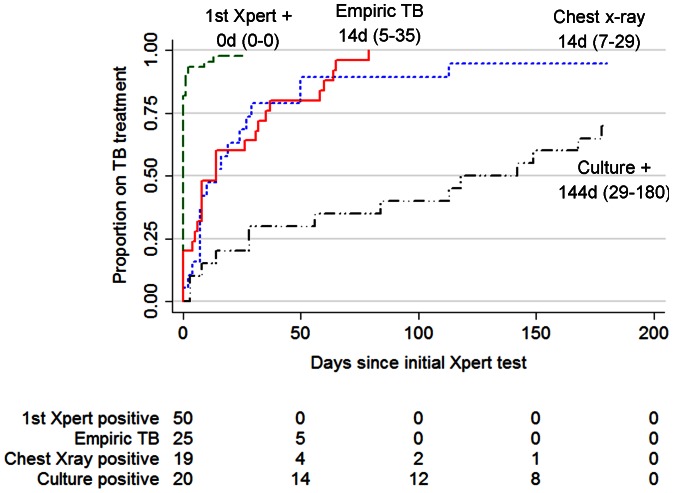
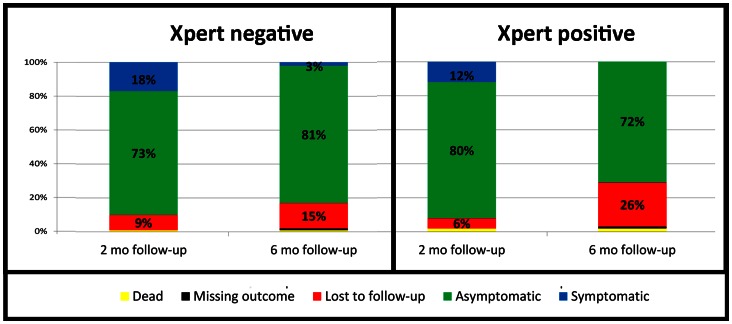
Results: From July-September 2011, 641 tuberculosis suspects were enrolled, of whom 69% were HIV-infected. Eight percent were positive by a single Xpert. Among 116 individuals diagnosed with TB, 66 (57%) were Xpert negative, of which 44 (67%) were empirical or radiological diagnoses and 22 (33%) were Xpert negative/culture-positive. The median time to tuberculosis treatment was 0 days (IQR: 0-0) for Xpert positives, 14 days (IQR: 5-35) for those diagnosed empirically, 14 days (IQR: 7-29) for radiological diagnoses, and 144 days (IQR: 28-180) for culture positives. Xpert negative tuberculosis cases were clinically similar to Xpert positives, including HIV status and CD4 count, and had similar treatment outcomes including mortality and time to antiretroviral treatment initiation.
Conclusions: In a high HIV-burden setting, a single Xpert identified less than half of those started on tuberculosis treatment, highlighting the complexity of TB diagnosis even in the Xpert era. Xpert at point-of-care resulted in same day treatment initiation in Xpert-positives, but had no impact on tuberculosis treatment outcomes or mortality.
Conflict of interest statement
Figures
References
-
- WHO (2011) Global Tuberculosis Control. Geneva.
-
- Chang K, Lu W, Wang J, Zhang K, Jia S, et al. (2012) Rapid and effective diagnosis of tuberculosis and rifampicin resistance with Xpert MTB/RIF assay: a meta-analysis. J Infect 64: 580–588. - PubMed
-
- WHO (2011) Policy statement: automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Xpert MTB/RIF system. Geneva, Switzerland. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
