

doi: 10.5402/2012/238505.
Print 2012.
Imaging evaluation of dogs and cats with Dysphagia
Affiliations
- PMID: 23762579
- PMCID: PMC3671744
- DOI: 10.5402/2012/238505
Item in Clipboard
Imaging evaluation of dogs and cats with Dysphagia
ISRN Vet Sci.
.
Abstract
The current literature is reviewed in this paper regarding the application of diagnostic imaging in the evaluation of swallowing disorders of the dog. The applications of radiography, contrast radiography, and contrast videofluoroscopy are discussed with pertinent case examples provided for emphasis. The indications for image-guided interventions are also described.
Figures
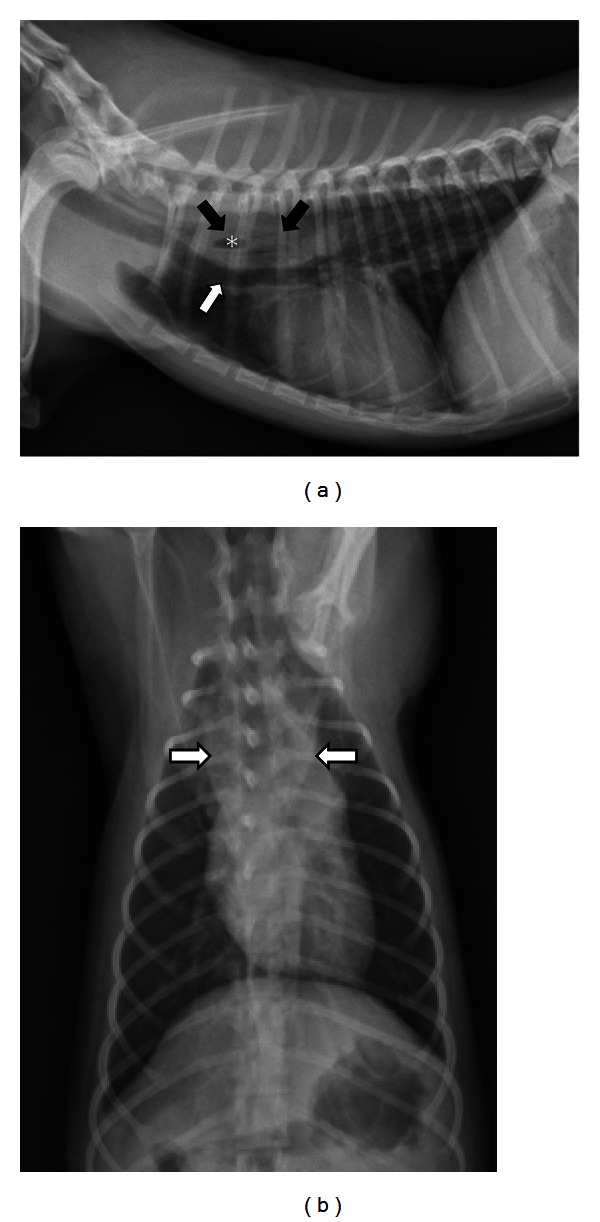
(a) A right lateral thoracic radiograph depicts a 1-year-old spayed female Yorkshire terrier with an acute onset of retching and regurgitation. A rawhide foreign body is present in the cranial thoracic esophagus (black arrows). Notice that the foreign body is difficult to see because raw hide is soft tissue density but a gas bubble in the middle is visible (∗). The distended esophagus is pushing the trachea ventrally (white arrow). There is a small amount of air in the esophagus oral to the obstruction. (b) A dorsoventral radiograph of the same dog as in (a) shows widening of the esophagus in the location of the foreign body (white arrows).
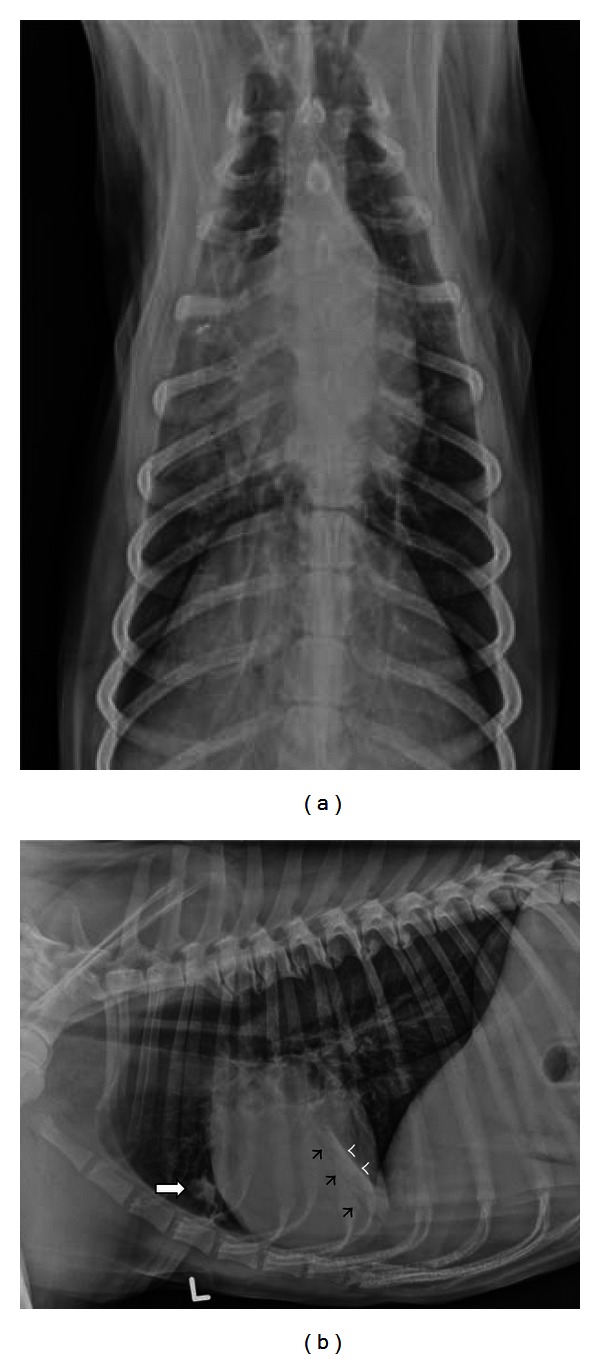
(a) A dorsoventral radiograph depicts a 4-year-old spayed female Collie with dysphagia. Alveolar infiltrates with air bronchogram formation are seen in the right cranial and middle lung lobes. (b) A left lateral radiograph of the same dog as in (a) confirms dependent pulmonary infiltrates consistent with aspiration pneumonia in the right cranial (white arrow) and right middle lung lobes. Air bronchogram formation (black arrowheads) and a lobar margin (white arrowheads) define alveolar density in the right middle lung lobe.
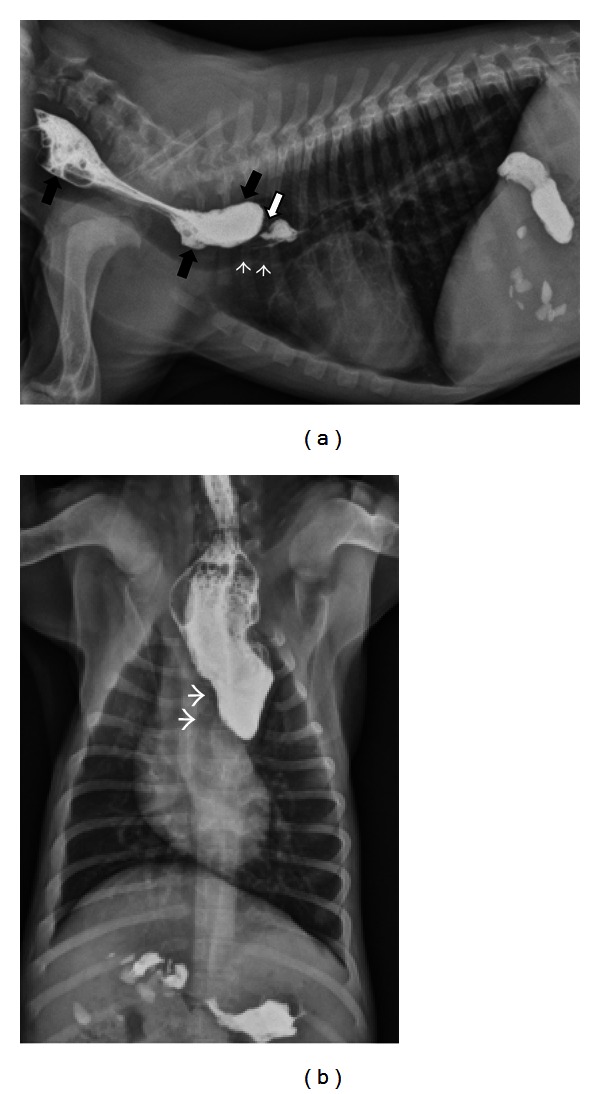
(a) A right lateral thoracic radiograph depicts a 2-month-old male Labrador presenting for regurgitation starting after weaning. Liquid barium has been administered orally immediately prior to radiography. There is a focal narrowing of the esophageal luminal diameter immediately dorsal to the heart base (white arrow). The trachea undulates and deviates ventrally in the same region (white arrowheads). Contrast is pooling is a dilated esophagus oral to the lesion (black arrows). (b) A dorsoventral radiograph of the same dog as in (a) shows contrast dilation of the cervical esophagus and an abrupt termination of the contrast column at the heart base. The trachea deviates to the left (white arrowheads) as is typically seen with persistent right aortic arch.
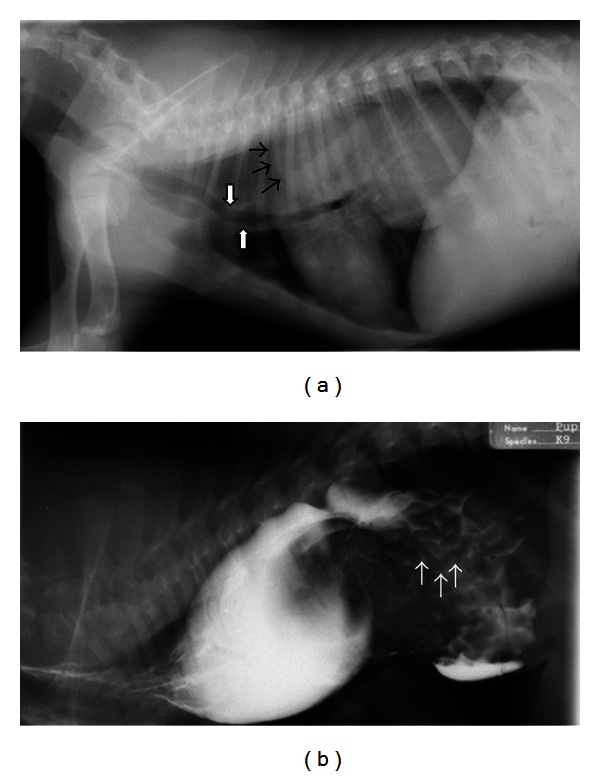
(a) A right lateral thoracic radiograph shows a 3-month-old male German Shepherd presenting for regurgitation and retching. There is gas distention of the cranial thoracic esophagus and a large soft tissue dense mass visible in the caudal dorsal thorax. A gas-soft tissue interface is seen at the cranial margin of the mass (black arrows) indicating that the mass resides within the esophagus. The trachea is displaced ventrally (white arrows). The stomach is not visualized in the abdomen. (b) A right lateral thoracic radiograph of the same dog as in (a) following the administration of liquid barium confirms that the mass is in the esophagus. There are rugal folds on the surface of the mass (white arrows) verifying the diagnosis of gastroesophageal intussusception.
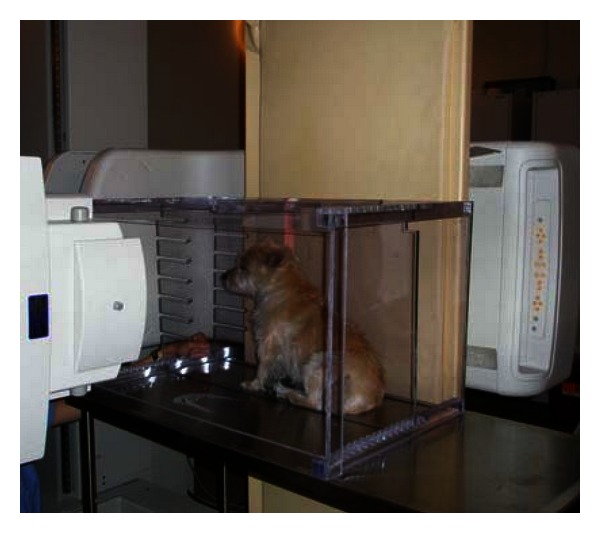
A plexiglass box is used to restrain this dog in the sitting or standing position. The X-ray source is aimed horizontally through the positioning box toward the detector located within the fluoroscopy table.
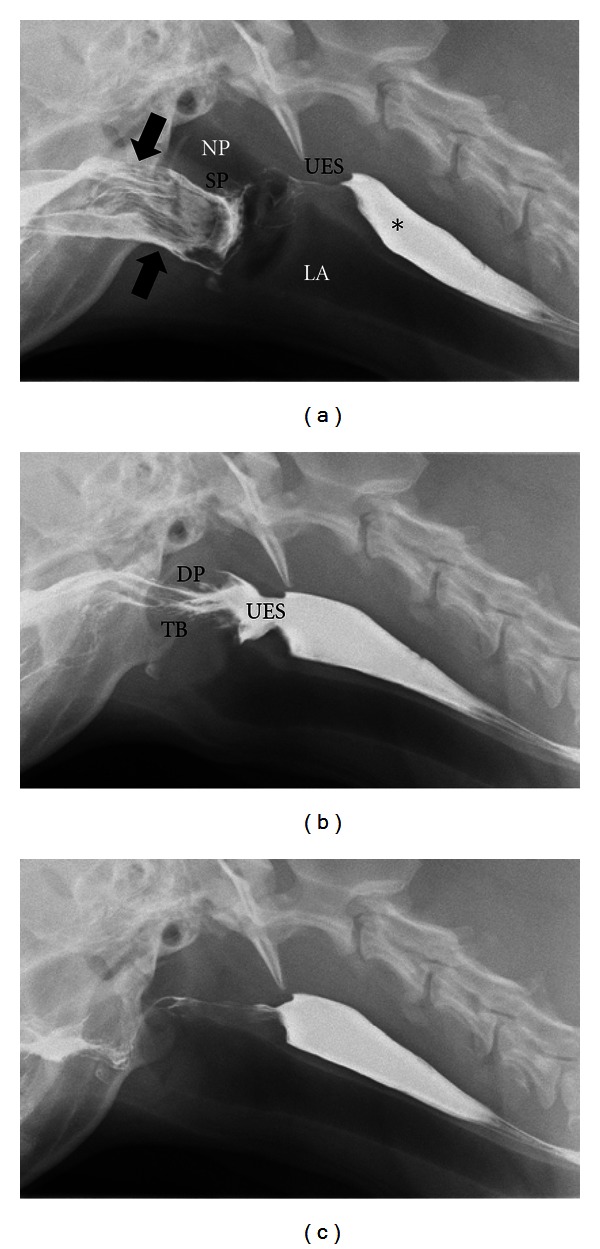
Digitally captured fluoroscopic images are shown from a 5-year-old female Golden Retriever with no evidence of dysphagia. (a) This image is taken as the dog laps barium that is placed into the mouth using a catheter tipped syringe but before swallowing is initiated. Barium contrast medium is present in the oral cavity (black arrows) with some residual barium in the proximal esophagus from the previous swallow (∗). NP = nasopharynx; LA = larynx; SP = soft palate; UES = upper esophageal sphincter. (b) The dorsal pharyngeal wall (DP) contracts ventrally to meet the tongue base (TB) and propels the liquid contrast medium caudally toward the upper esophageal sphincter (UES). The UES is wide open in coordination with caudal bolus propulsion. (c) After the bolus passes through the UES and the swallow is complete, only minimal barium remains in the oral cavity. An esophageal wave will propel the bolus from the proximal esophagus to the stomach.
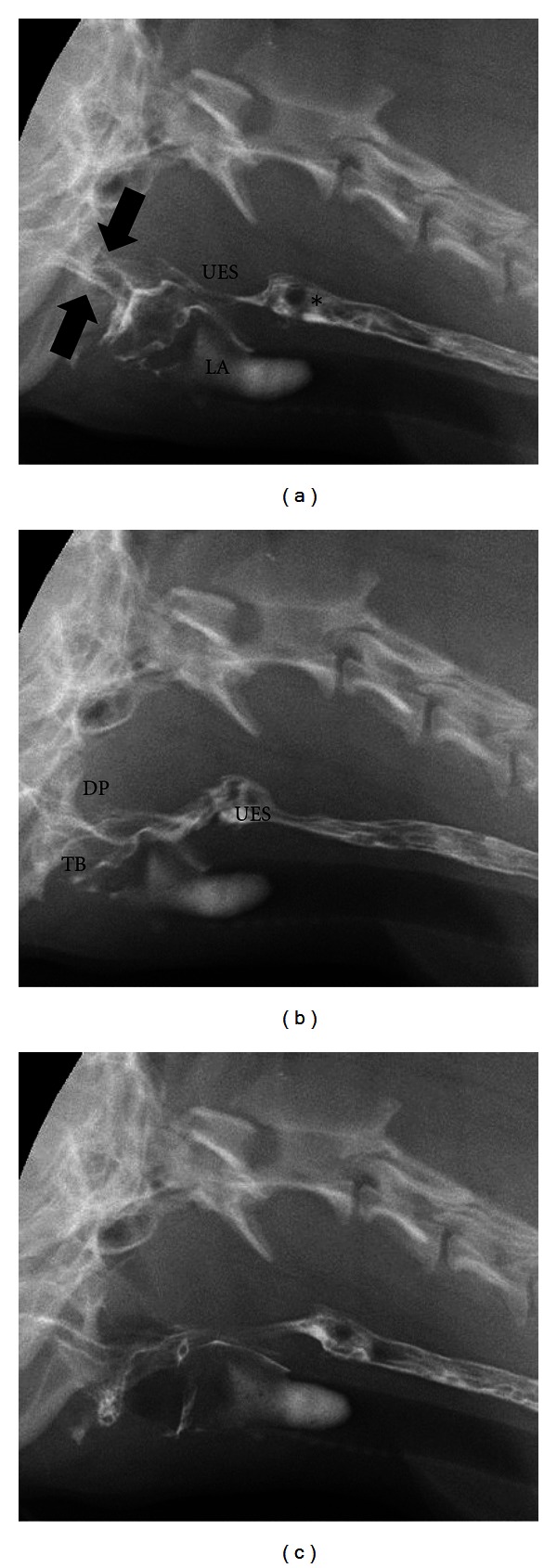
Digitally captured fluoroscopic images are shown from a 2-year-old castrated male Cavalier King Charles Spaniel with pharyngeal weakness related to immune mediated polymyositis. (a) This image is taken as the dog laps barium that is placed into the mouth using a catheter tipped syringe but before swallowing is initiated. A small quantity of barium contrast medium is present in the oral cavity (black arrows) with some residual barium in the proximal esophagus from the previous swallow (∗). Aspirated barium is also seen in the larynx (LA) and proximal trachea. UES = upper esophageal sphincter. (b) The dorsal pharyngeal wall (DP) contracts ventrally to meet the tongue base (TB) but bolus propulsion is lazy and incomplete. The upper esophageal sphincter (UES) opens in a timely manner in relation to pharyngeal contraction. (c) After the bolus passes through the UES and the swallow is complete a moderate quantity of barium remains in the oral cavity.
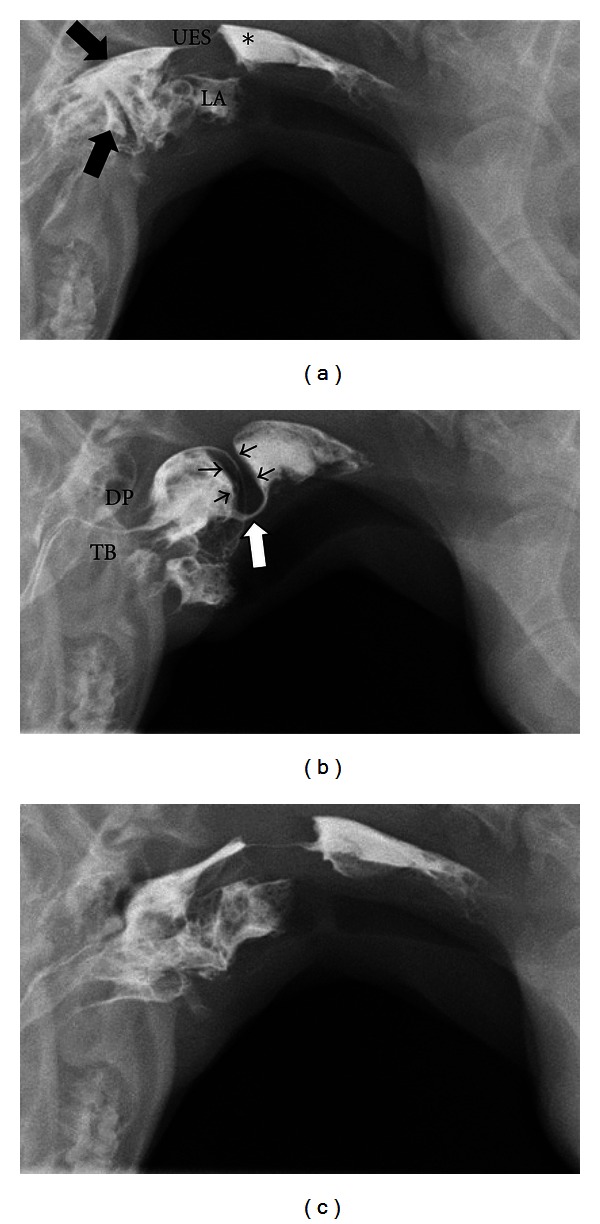
Digitally captured fluoroscopic images are shown from a 6-month-old spayed female miniature Dachshund with cricopharyngeal achalasia. (a) This image is taken as the dog laps barium that is placed into the mouth using a catheter tipped syringe but before swallowing is initiated. A moderate quantity of barium contrast medium is present in the oral cavity (black arrows) with some residual barium in the proximal esophagus from the previous swallow (∗). Aspirated barium is also seen in the larynx (LA) and proximal trachea. UES = upper esophageal sphincter. (b) The dorsal pharyngeal wall (DP) contracts ventrally vigorously to meet the tongue base (TB) but bolus passage is obstructed by a hypertrophied cricopharyngeous muscle (black arrowheads). The upper esophageal sphincter (white arrow) attempts to open in coordination with caudal bolus propulsion but the luminal diameter is extremely narrow. (c) After the bolus passes through the UES and the swallow is complete a moderate quantity of barium remains in the oral cavity.
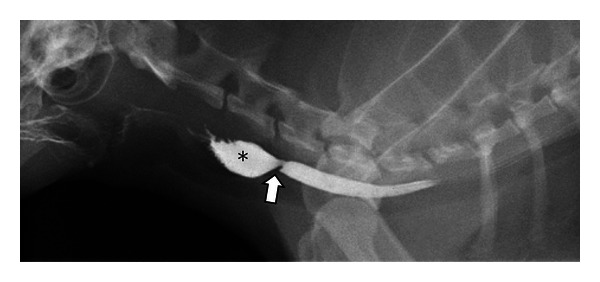
A digitally captured fluoroscopic image is shown from a 10-year-old spayed female domestic long-haired cat that presents with regurgitation following oral doxycycline therapy. Barium contrast medium has been administered and is filling the cervical esophagus. A focal narrowed region (white arrow) persists in the mid cervical esophagus. The esophageal lumen is dilated oral to the stricture (∗).
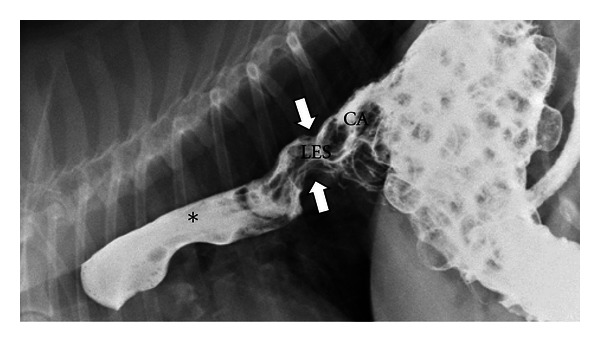
A digitally captured fluoroscopic image is shown from a 7-year-old spayed female Beagle that presents with chronic regurgitation. Liquid barium and barium soaked kibble has been administered. The lower esophageal sphincter (LES) is seen to be displaced cranial to the diaphragm and into the thoracic cavity (white arrow) and is pulling the gastric cardia (CA) with it. Liquid barium is seen to reflux from the stomach into the thoracic esophagus (∗) secondary to this Type I hiatal hernia.
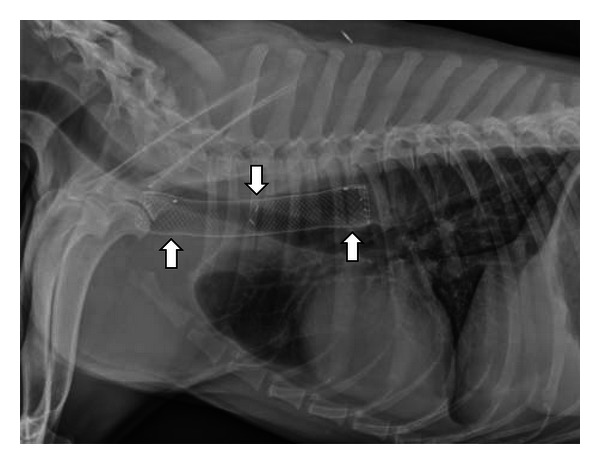
This right lateral thoracic radiograph was obtained from a 3-year-old spayed female Labrador Retriever who began regurgitating following a dental procedure. A benign stricture was diagnosed and treated with palliative stent placement when balloon dilation failed. The metallic mesh self-expanding stent is seen within the cranial thoracic esophagus (white arrows).
References
-
- Watrous BJ. Clinical presentation and diagnosis of dysphagia. Veterinary Clinics of North America—Small Animal Practice. 1983;13(3):437–459. - PubMed
-
- Watrous BJ, Suter PF. Normal swallowing in the dog: a cineradiographic study. Veterinary Radiology and Ultrasound. 1979;20(3–6):99–109.
-
- Warnock JJ, Marks SL, Pollard R, Kyles AE, Davidson A. Surgical management of cricopharyngeal dysphagia in dogs: 14 cases (1989–2001) Journal of the American Veterinary Medical Association. 2003;223(10):1462–1468. - PubMed
-
- Watrous BJ. The esophagus. In: Thrall DE, editor. Veterinary Diagnostic Radiology. 5th edition. St. Louis, Mo, USA: Saunders Elsevier; 2007. pp. 495–511.
-
- Gengler W. Gagging. In: Ettinger SJ, Feldman EC, editors. The Textbook of Veterinary Internal Medicine. St Louis, Mo, USA: Saunders Elsevier; 2010. pp. 189–191.
LinkOut - more resources
Full Text Sources
Miscellaneous
