

Demyelinating Disease following Anti-TNFa Treatment: A Causal or Coincidental Association? Report of Four Cases and Review of the Literature
- PMID: 23762678
- PMCID: PMC3670521
- DOI: 10.1155/2013/671935
Demyelinating Disease following Anti-TNFa Treatment: A Causal or Coincidental Association? Report of Four Cases and Review of the Literature
Abstract
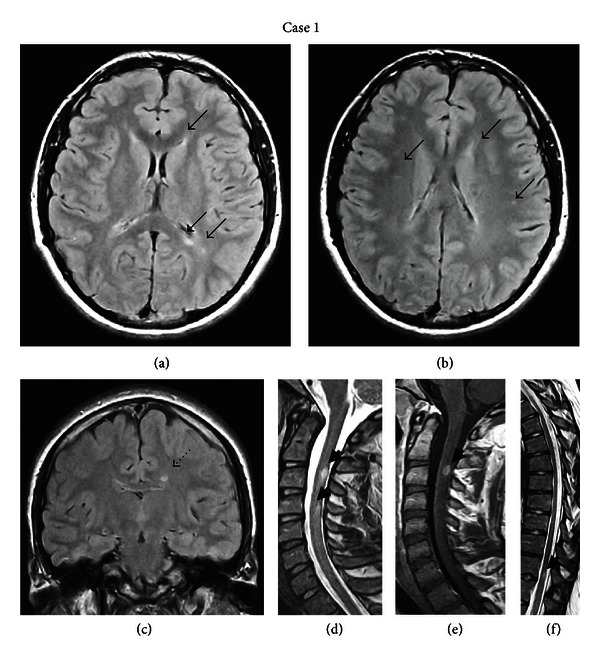
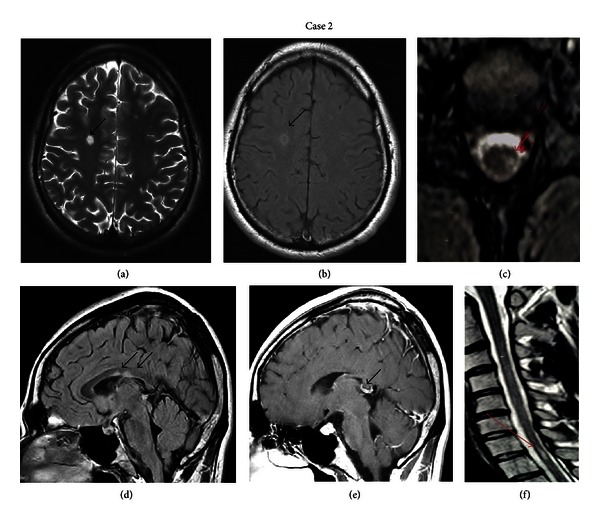
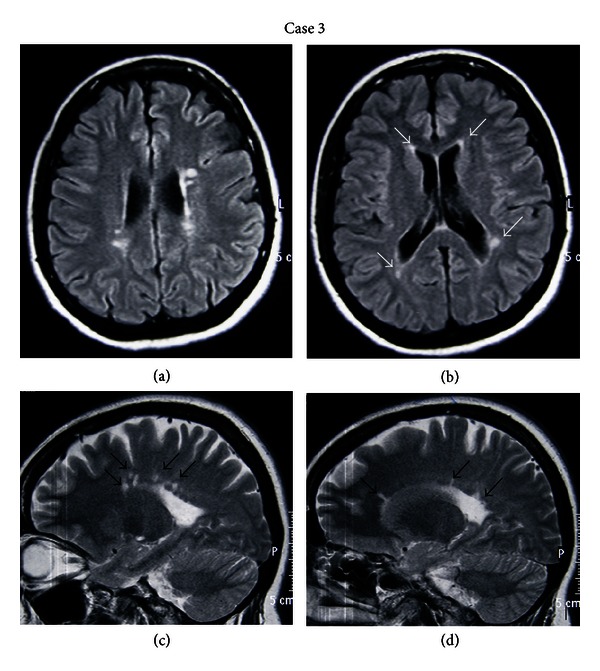
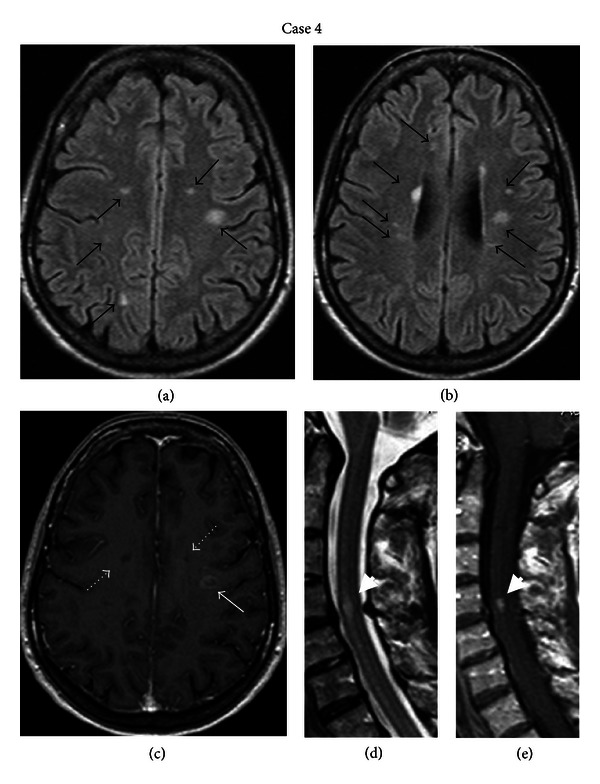
Tumor necrosis factor antagonists (anti-TNFa) are an established therapeutic option for several autoimmune and inflammatory bowel diseases. Despite their clinical effectiveness, neurological adverse events have been reported and literature data suggest a potential role of anti-TNFa in the induction of demyelination of the CNS. We present four patients treated with anti-TNFa who developed symptoms suggestive of CNS demyelination. The first patient, a 17-year-old male who received etanercept for psoriatic arthritis for eight months, presented with dysesthesias up to T4 level. The second patient, a 30-year-old male treated with adalimumab for three years due to ankylosing spondylitis, presented with right unilateral tinnitus. The third case, a 47-year-old female, received etanercept for four years because of psoriatic arthritis and developed persistent headache and left-sided face and head numbness. Finally, the fourth patient, a 57-years-old female treated with etanercept for six years due to ankylosing spondylitis, presented with difficulty in speech, swallowing, and ptosis of the right corner of the mouth. In all cases, brain MRI showed lesions suggestive of demyelination, while positive oligoclonal bands were detected in the CSF. Anti-TNFa treatments were discontinued and patients showed clinical improvement with pulsed intravenous corticosteroid therapy. CNS demyelination following anti-TNFa treatment represents a relatively rare but potential serious complication. Close follow-up and MRI monitoring of these patients is mandatory to elucidate whether the clinical manifestations represent adverse events occurring during anti-TNFa therapy or a first demyelinating episode.
Figures
References
-
- Tracey D, Klareskog L, Sasso EH, Salfeld JG, Tak PP. Tumor necrosis factor antagonist mechanisms of action: a comprehensive review. Pharmacology and Therapeutics. 2008;117(2):244–279. - PubMed
-
- Sfikakis PP, Tsokos GC. Towards the next generation of anti-TNF drugs. Clinical Immunology. 2011;141(3):231–235. - PubMed
-
- Kollias G, Douni E, Kassiotis G, Kontoyiannis D. On the role of tumor necrosis factor and receptors in models of multiorgan failure, rheumatoid arthritis, multiple sclerosis and inflammatory bowel disease. Immunological Reviews. 1999;169:175–194. - PubMed
-
- Caminero A, Comabella M, Montalban X. Tumor necrosis factor alpha (TNF-α), anti-TNF-α and demyelination revisited: an ongoing story. Journal of Neuroimmunology. 2011;234(1-2):1–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
