

Promoting universal financial protection: a case study of new management of community health insurance in Tanzania
- PMID: 23763711
- PMCID: PMC3686629
- DOI: 10.1186/1478-4505-11-21
Promoting universal financial protection: a case study of new management of community health insurance in Tanzania
Abstract
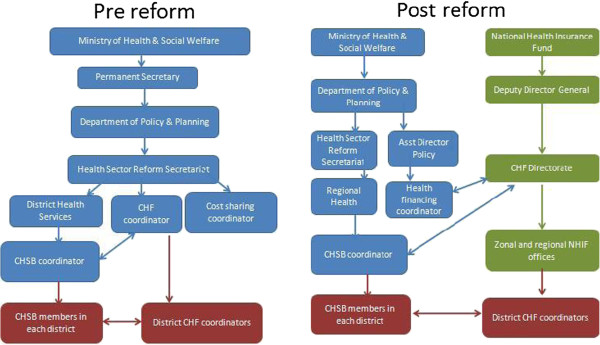
Background: The National Health Insurance Fund (NHIF), a compulsory formal sector scheme took over the management of the Community Health Fund (CHF), a voluntary informal sector scheme, in 2009. This study assesses the origins of the reform, its effect on management and reporting structures, financial flow adequacy, reform communication and acceptability to key stakeholders, and initial progress towards universal coverage.
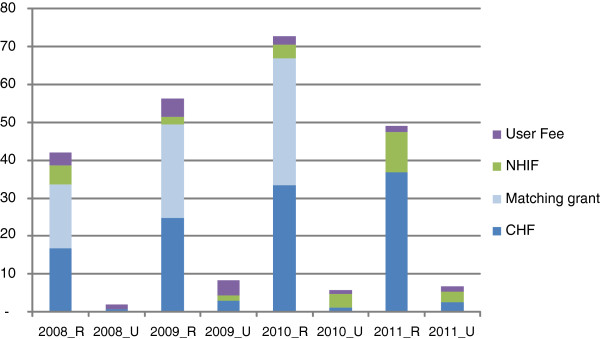
Methods: The study relied on national data sources and an in-depth collective case study of a rural and an urban district to assess awareness and acceptability of the reform, and fund availability and use relative to need in a sample of facilities.
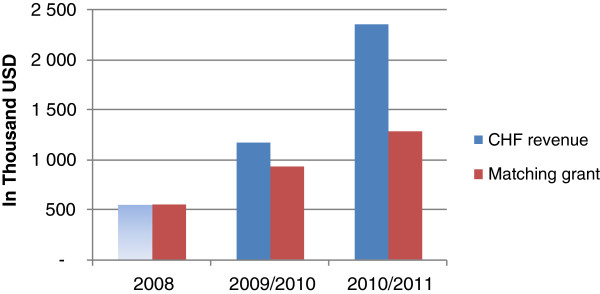
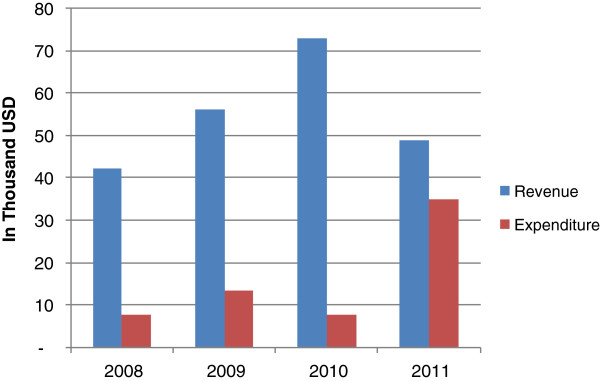
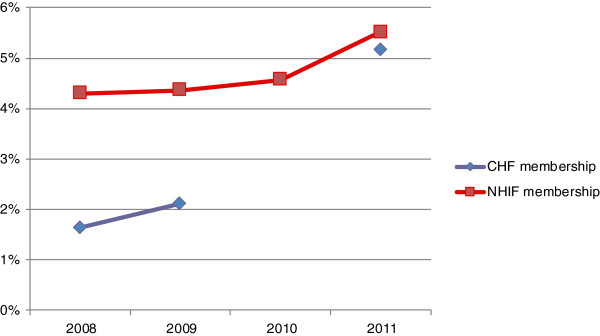
Results: The reform was driven by a national desire to expand coverage and increase access to services. Despite initial delays, the CHF has been embedded within the NHIF organisational structure, bringing more intensive and qualified supervision closer to the district. National CHF membership has more than doubled. However, awareness of the reform was limited below the district level due to the reform's top-down nature. The reform was generally acceptable to key stakeholders, who expected that benefits between schemes would be harmonised.The reform was unable to institute changes to the CHF design or district management structures because it has so far been unable to change CHF legislation which also limits facility capacity to use CHF revenue. Further, revenue generated is currently insufficient to offset treatment and administration costs, and the reform did not improve the revenue to cost ratio. Administrative costs are also likely to have increased as a result of the reform.
Conclusion: Informal sector schemes can benefit from merger with formal sector schemes through improved data systems, supervision, and management support. However, effects will be maximised if legal frameworks can be harmonised early on and a reduction in administrative costs is not guaranteed.
Figures
References
-
- McIntyre D, Garshong B, Mtei G, Meheus F, Thiede M, Akazili J, Ally M, Aikins M, Mulligan JA, Goudge J. Beyond fragmentation and towards universal coverage: insights from Ghana, South Africa and the United Republic of Tanzania. Bull World Health Organ. 2008;86(11):871–876. doi: 10.2471/BLT.08.053413. - DOI - PMC - PubMed
-
- Mtei GJ, Mulligan M, Ally N, Palmer A. Mills: An Assessment of the Health Financing System in Tanzania. Dar es Salaam: Ifakara Health Institute; 2007.
-
- International Social Security Association. Dynamic Social Security for Africa: Extending social protection for development. Social Policy Highlight 07. 2008. http://www.issa.int/Resources/Social-Policy-Highlight/Dynamic-Social-Sec....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
