

Predictive, preventive, personalised and participatory periodontology: 'the 5Ps age' has already started
- PMID: 23763842
- PMCID: PMC3703280
- DOI: 10.1186/1878-5085-4-16
Predictive, preventive, personalised and participatory periodontology: 'the 5Ps age' has already started
Abstract
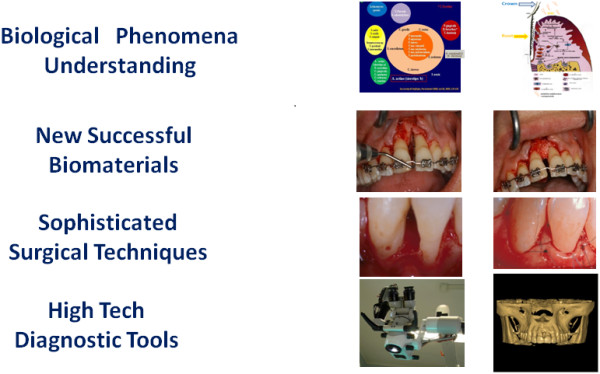
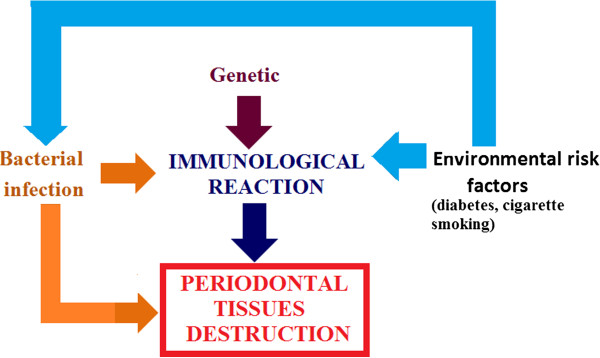
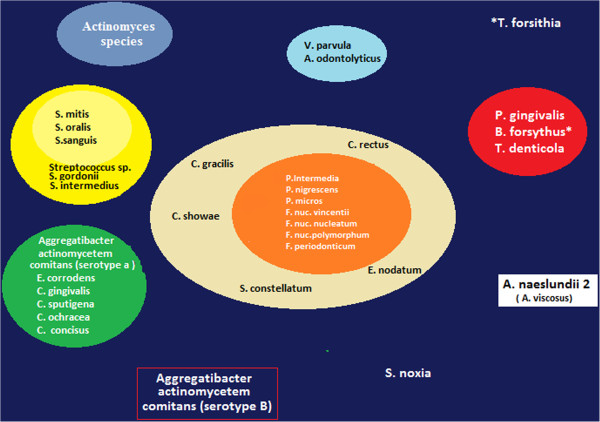
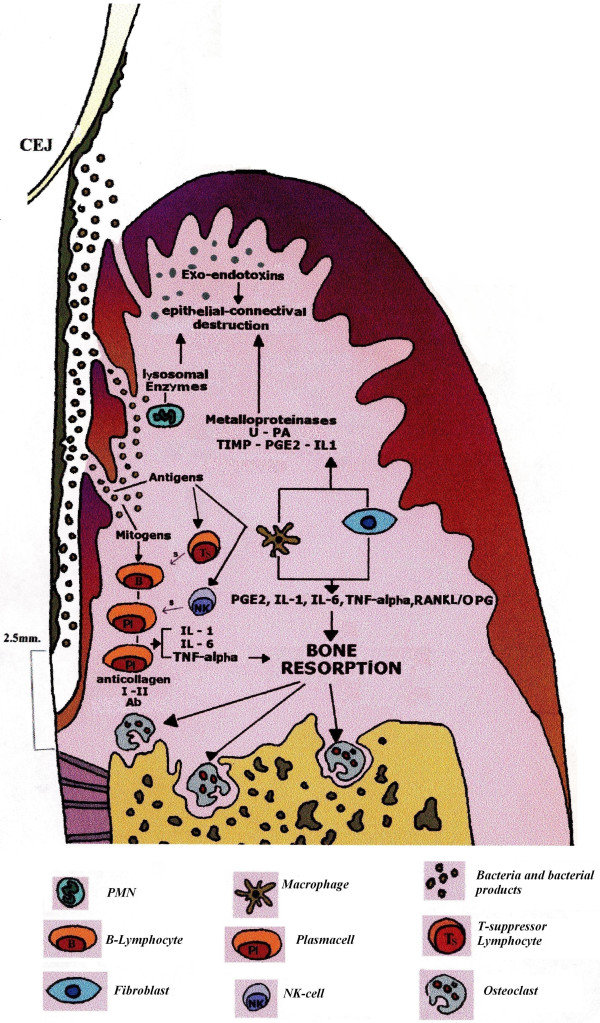
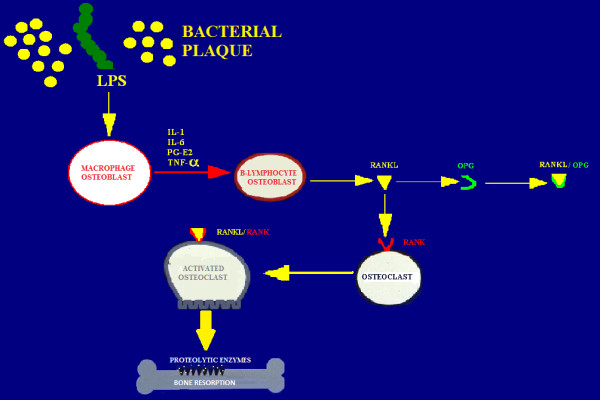
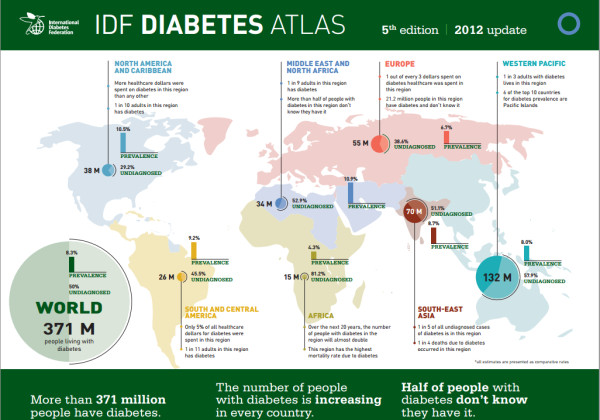
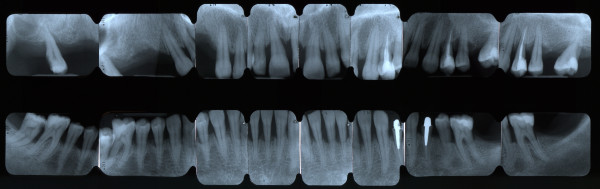
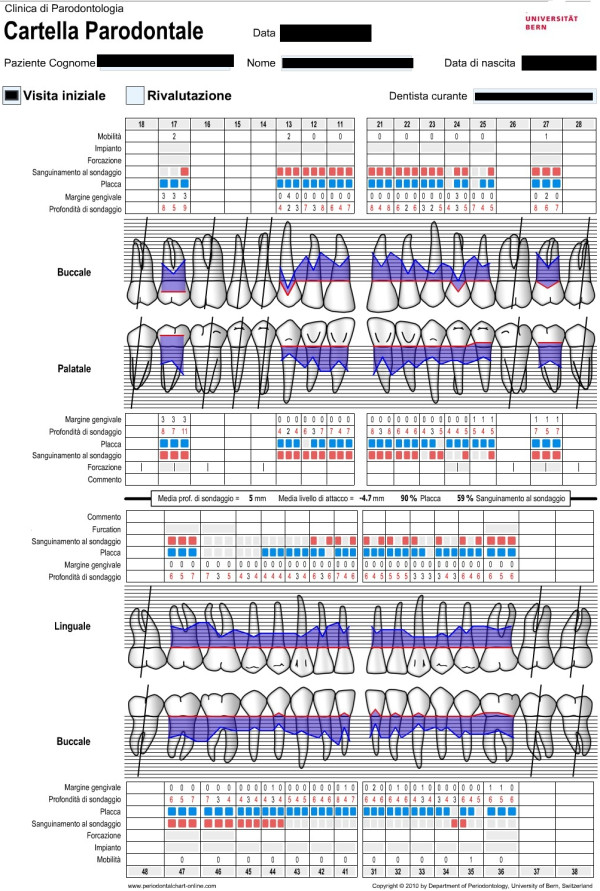
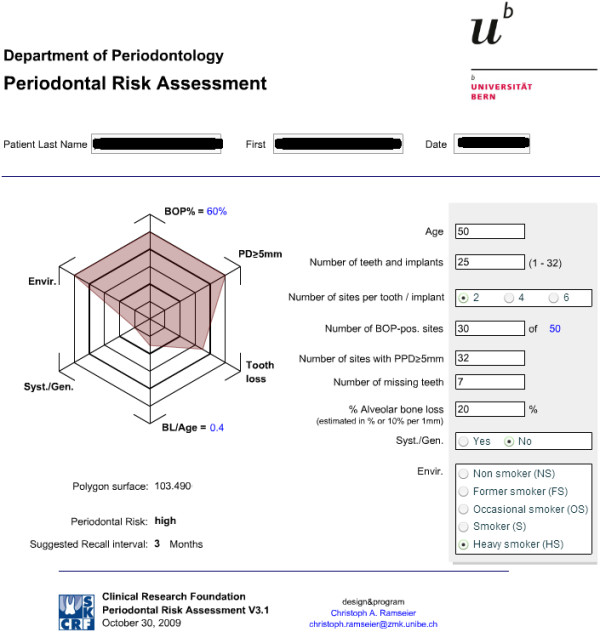
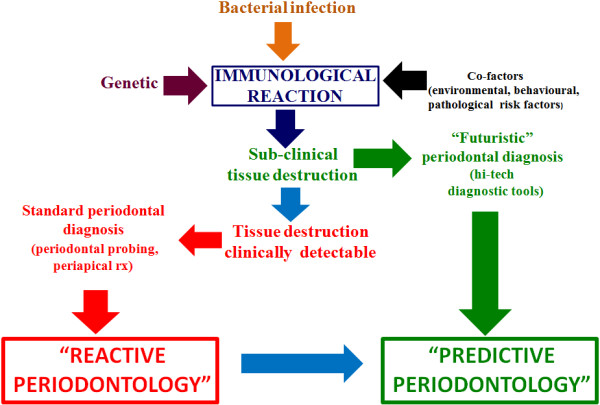
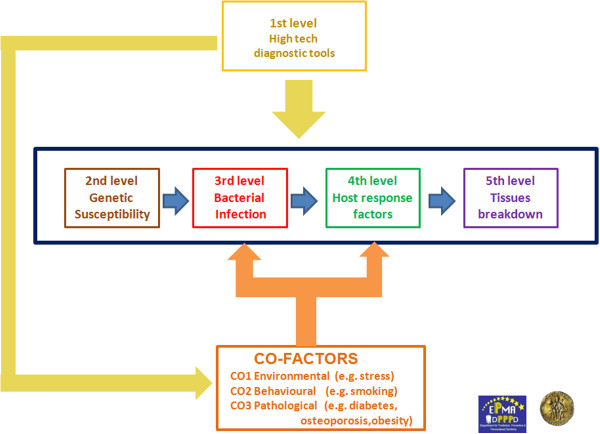
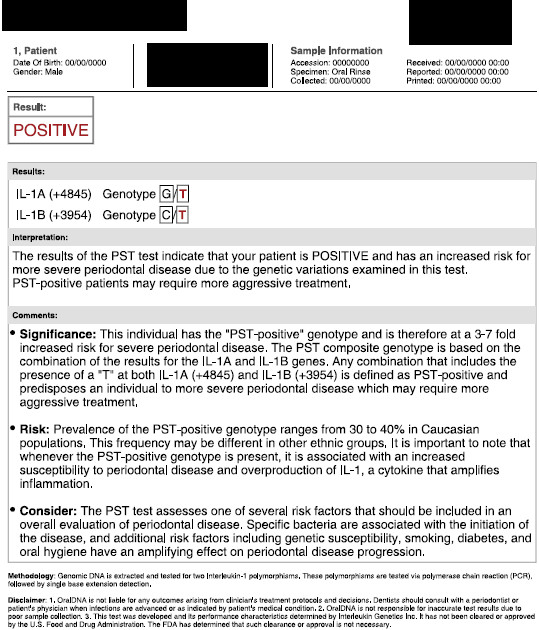
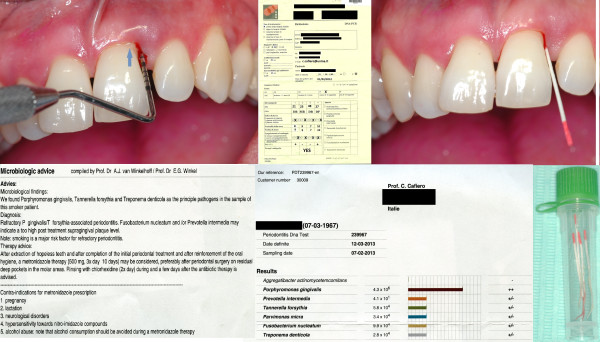
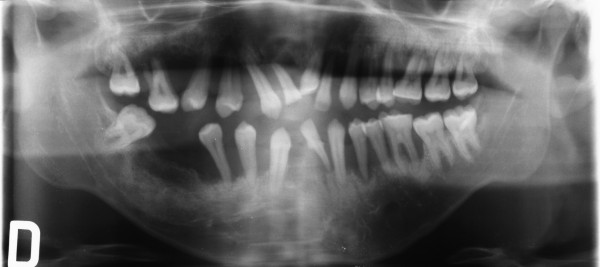
An impressive progress in dentistry has been recorded in the last decades. In order to reconsider guidelines in dentistry, it is required to introduce new concepts of personalised patient treatments: the wave of predictive, preventive and personalised medicine is rapidly incoming in dentistry. Worldwide dentists have to make a big cultural effort in changing the actual 'reactive' therapeutic point of view, belonging to the last century, into a futuristic 'predictive' one. The first cause of tooth loss in industrialised world is periodontitis, a Gram-negative anaerobic infection whose pathogenesis is genetically determined and characterised by complex immune reactions. Chairside diagnostic tests based on saliva, gingival crevicular fluid and cell sampling are going to be routinely used by periodontists for a new approach to the diagnosis, monitoring, prognosis and management of periodontal patients. The futuristic '5Ps' (predictive, preventive, personalised and participatory periodontology) focuses on early integrated diagnosis (genetic, microbiology, host-derived biomarker detection) and on the active role of the patient in which networked patients will shift from being mere passengers to responsible drivers of their health. In this paper, we intend to propose five diagnostic levels (high-tech diagnostic tools, genetic susceptibility, bacterial infection, host response factors and tissue breakdown-derived products) to be evaluated with the intention to obtain a clear picture of the vulnerability of a single individual to periodontitis in order to organise patient stratification in different categories of risk. Lab-on-a-chip (LOC) technology may soon become an important part of efforts to improve worldwide periodontal health in developed nations as well as in the underserved communities, resource-poor areas and poor countries. The use of LOC devices for periodontal inspection will allow patients to be screened for periodontal diseases in settings other than the periodontist practice, such as at general practitioners, general dentists or dental hygienists. Personalised therapy tailored with respect to the particular medical reality of the specific stratified patient will be the ultimate target to be realised by the 5Ps approach. A long distance has to be covered to reach the above targets, but the pathway has already been clearly outlined.
Figures














References
-
- European Association for Predictive, Preventive and Personalised Medicine - EPMA. [ http://www.epmanet.eu]
-
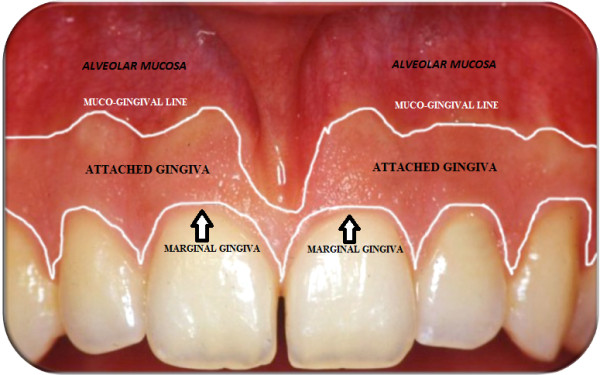
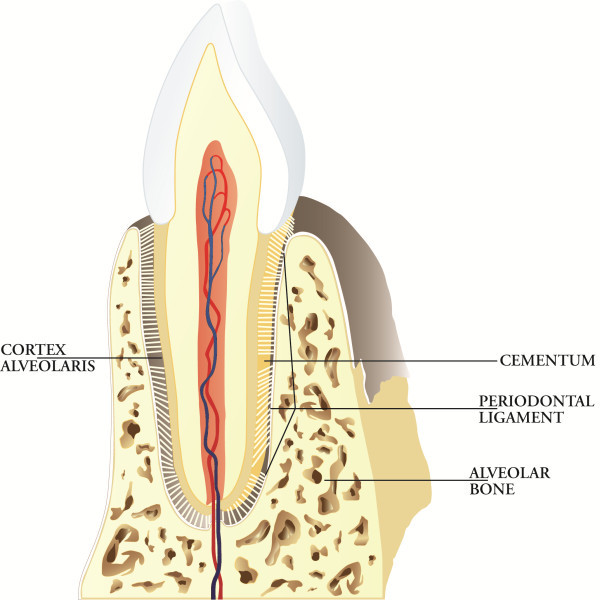
- Lindhe J, Lang NP, Karring T. In: Clinical Periodontology and Implant Dentistry. Volume 1. 5. Lindhe J, Karring T, Araujo M, editor. Copenhagen: Blackwell Munksgaard; 2008. The anatomy of periodontal tissue; pp. 3–48.
-
- Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999;4:1–6. - PubMed
-
- Socransky SS. Microbiology of periodontal disease – present status and future considerations. J Periodontol. 1977;48(9):497–504. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
