

Clinical usefulness of response profiles to rapidly incremental cardiopulmonary exercise testing
- PMID: 23766901
- PMCID: PMC3666297
- DOI: 10.1155/2013/359021
Clinical usefulness of response profiles to rapidly incremental cardiopulmonary exercise testing
Abstract
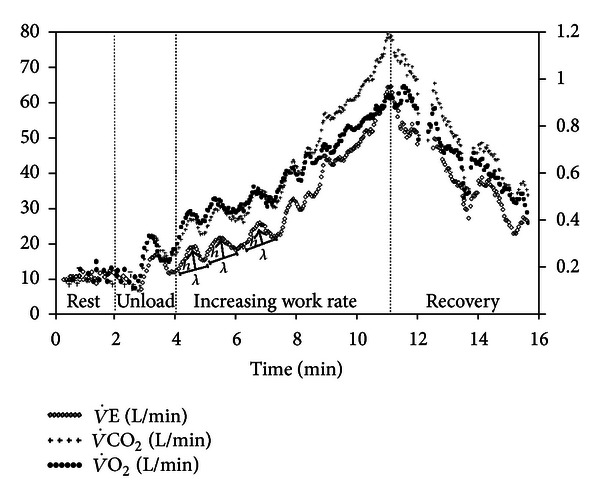
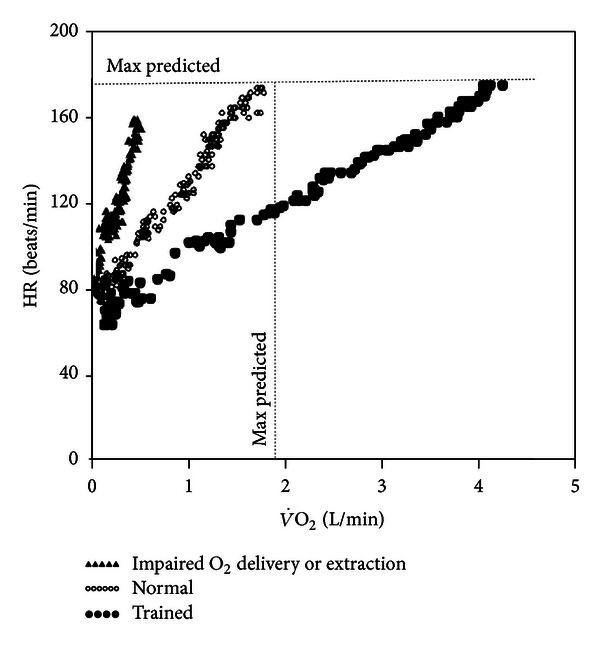
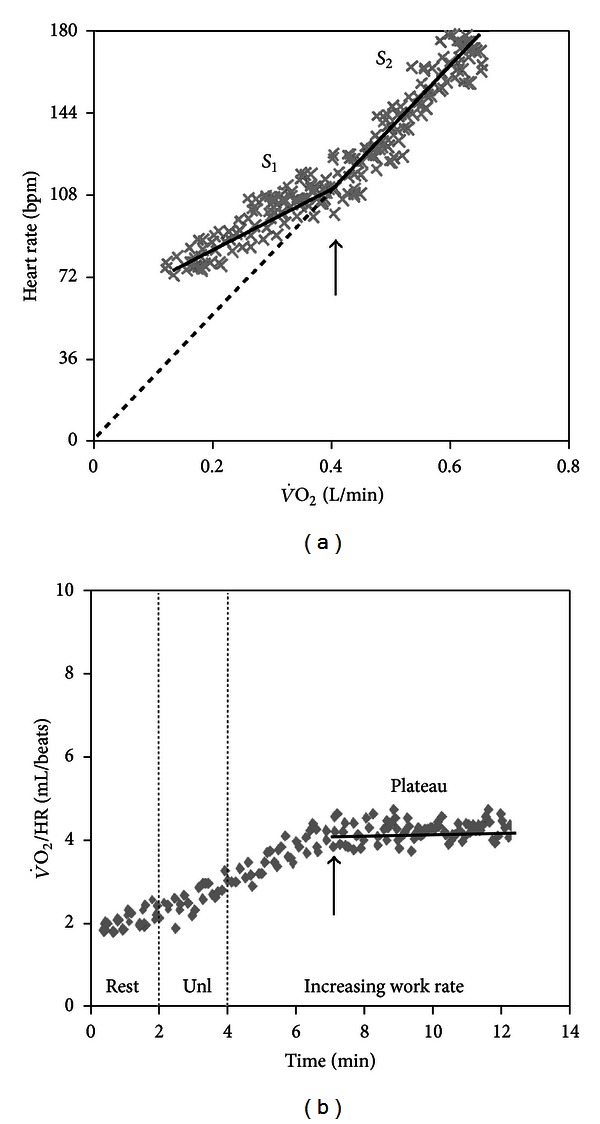
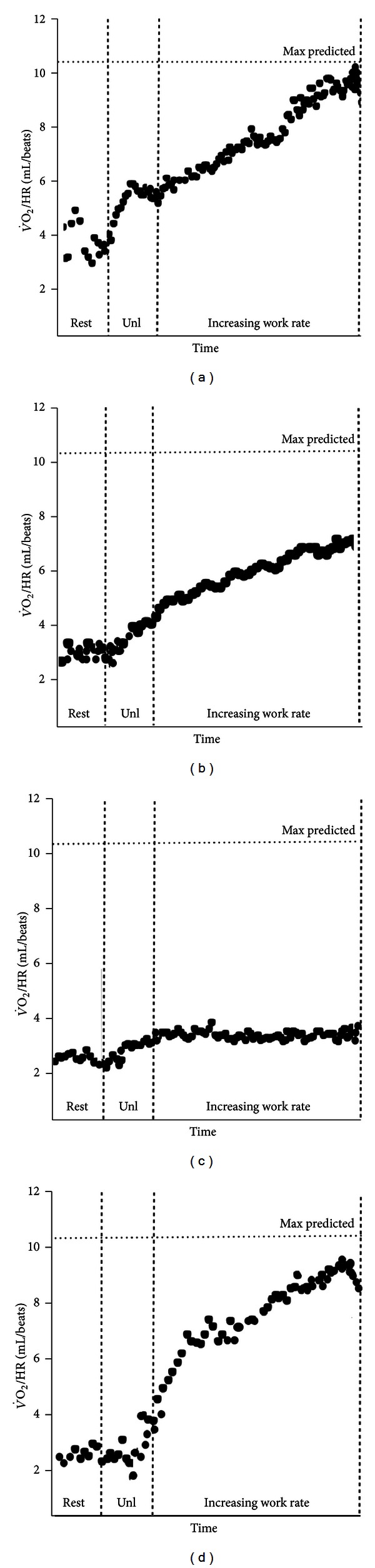
The advent of microprocessed "metabolic carts" and rapidly incremental protocols greatly expanded the clinical applications of cardiopulmonary exercise testing (CPET). The response normalcy to CPET is more commonly appreciated at discrete time points, for example, at the estimated lactate threshold and at peak exercise. Analysis of the response profiles of cardiopulmonary responses at submaximal exercise and recovery, however, might show abnormal physiologic functioning which would not be otherwise unraveled. Although this approach has long been advocated as a key element of the investigational strategy, it remains largely neglected in practice. The purpose of this paper, therefore, is to highlight the usefulness of selected submaximal metabolic, ventilatory, and cardiovascular variables in different clinical scenarios and patient populations. Special care is taken to physiologically justify their use to answer pertinent clinical questions and to the technical aspects that should be observed to improve responses' reproducibility and reliability. The most recent evidence in favor of (and against) these variables for diagnosis, impairment evaluation, and prognosis in systemic diseases is also critically discussed.
Figures

References
-
- Wasserman K, Whipp BJ. Exercise physiology in health and disease. The American Review of Respiratory Disease. 1975;112(2):219–249. - PubMed
-
- Wasserman K, Hansen JE, Sue DY, et al. Principles of Exercise Testing and Interpretation. 5th edition. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2012.
-
- Beaver WL, Wasserman K, Whipp BJ. On-line computer analysis and breath-by-breath graphical display of exercise function tests. Journal of Applied Physiology. 1973;34(1):128–132. - PubMed
-
- Whipp BJ, Davis JA, Torres F, Wasserman K. A test to determine parameters of aerobic function during exercise. Journal of Applied Physiology Respiratory Environmental and Exercise Physiology. 1981;50(1):217–221. - PubMed
-
- Buchfuhrer MJ, Hansen JE, Robinson TE, et al. Optimizing the exercise protocol for cardiopulmonary assessment. Journal of Applied Physiology Respiratory Environmental and Exercise Physiology. 1983;55(5):1558–1564. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
