

doi: 10.1016/j.eats.2012.07.005.
Print 2012 Dec.
Endoscopic proximal hamstring repair and ischial bursectomy
Affiliations
- PMID: 23766996
- PMCID: PMC3678643
- DOI: 10.1016/j.eats.2012.07.005
Item in Clipboard
Endoscopic proximal hamstring repair and ischial bursectomy
Arthrosc Tech.
.
Abstract
With the significant increase in use of the arthroscope around the hip have come several less invasive techniques to manage pathologies around this joint. This technical note with a video details one such technique that allows for the endoscopic management of proximal hamstring tears and chronic ischial bursitis, which until now have been managed exclusively with much larger open approaches. This procedure allows for complete exposure of the posterior aspect of the hip in a safe, minimally invasive fashion.
Figures
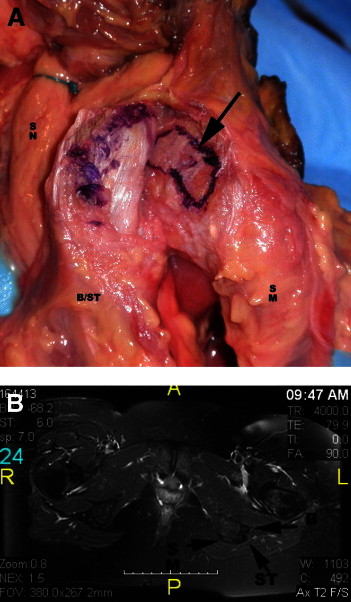
(A) Cadaveric dissection of the ischium in a left hip, viewed from the posterior aspect. The arrow points to the origin of the biceps/semitendinosus (B/ST), which has been elevated and retracted laterally. (B) Axial T2-weighted magnetic resonance image depicting the anatomy of the hamstring origin in a left hip. (B, biceps origin; SM, origin of semimembranosus; SN, sciatic nerve; ST, semitendinosus.)

Anteroposterior radiograph of the pelvis showing bilateral bony avulsions of the ischial tuberosities (arrows) in a 14-year-old athlete.
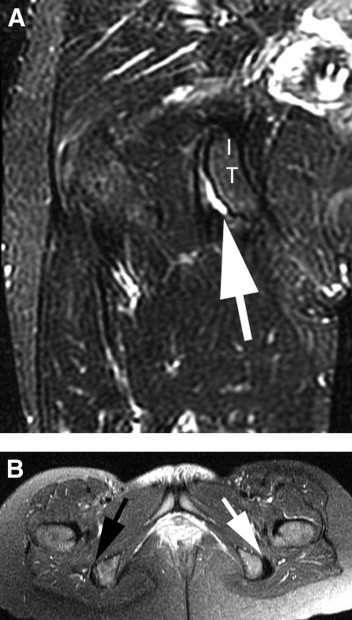
MRI views of a partial insertional tear with a sickle sign, indicating fluid within the ischial bursa. (A) A coronal T2-weighted view of a right hip showing the sickle sign (arrow). (IT, ischial tuberosity.) (B) Axial T2-weighted view showing both ischial tuberosities. One should note the right side (black arrow) showing the sickle sign and the normal left side (white arrow).

Image of patient positioned prone with the left hip and leg draped free.

Image of a left hip with the patient in the prone position showing the standard portals for endoscopic hamstring repair. The arthroscope is in the medial portal, and the shaver is in the distal portal.
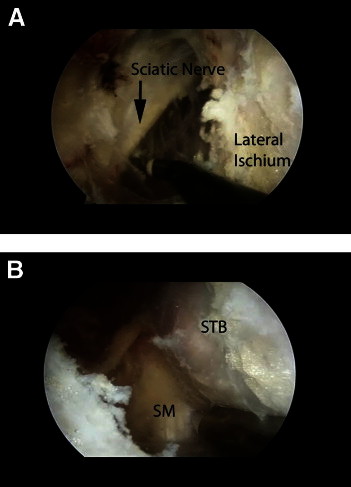
Endoscopic views of the subgluteal space in a left hip. The arthroscope is in the lateral portal. (A) With the instrument in the medial portal, a branch of the sciatic nerve has been exposed along with the lateral ischium. (B) The separate attachments of the semimembranosus (SM) tendon more anterior and lateral and the common biceps and semitendinosus (STB) tendon more posterior and medial.
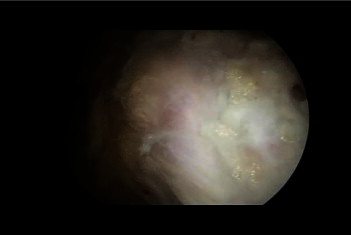
Endoscopic view of the proximal hamstring origin in a left hip with the arthroscope in the lateral portal. The distal end of the ischium has been cleared of soft tissue.
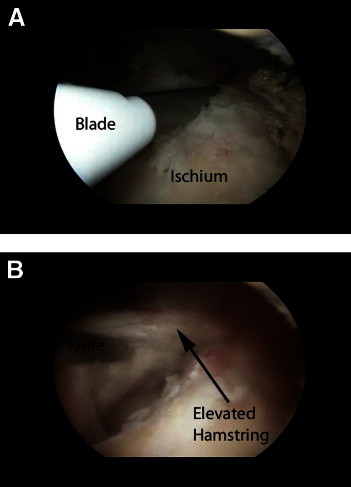
Endoscopic views of the proximal hamstring origin in a left hip with the arthroscope in the lateral portal. (A) A knife has been inserted through the distal portal, and the biceps-semitendinosus attachment has been incised. (B) The common biceps-semitendinosus origin has been elevated.
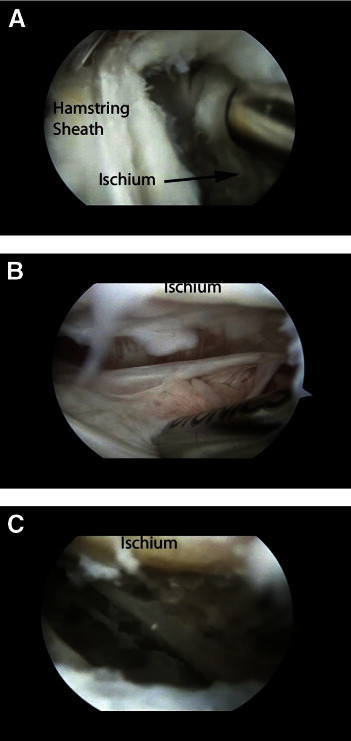
Endoscopic views of the proximal hamstring origin in a left hip with the arthroscope in the lateral portal. (A) The common biceps-semitendinosus origin has been incised and elevated. The tool serves to retract the detached tissue. (B) Ischial bursa before debridement. Hypertrophic inflammatory tissue is present in the bursal space. (C) Final debridement of bursa. The exposed bony surface at the top of the image should be noted.
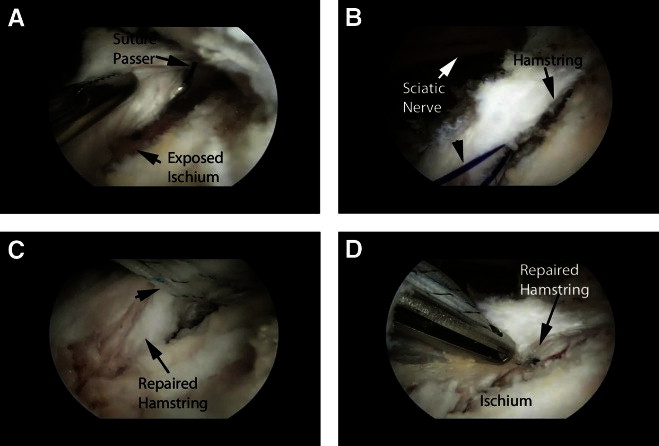
Endoscopic views of repair of the proximal hamstring origin in a left hip with the arthroscope in the lateral portal. (A) The ischium has been prepared, and the suture passer is in place. (B) Shuttle suture in place (arrowhead). The proximity of the sciatic nerve to the repair should be noted. (C) Final mattress sutures in place in the substance of the tendon (arrowheads). (D) Final tendon repair with the tendon edges reattached to the ischial footprint.
Comment in
-
Authors' reply.Arthroscopy. 2013 Nov;29(11):1738-9. doi: 10.1016/j.arthro.2013.08.028. Arthroscopy. 2013. PMID: 24209669 No abstract available.
-
Proximal origin of the hamstring muscle group.Arthroscopy. 2013 Nov;29(11):1738. doi: 10.1016/j.arthro.2013.08.029. Arthroscopy. 2013. PMID: 24209670 No abstract available.
References
-
- Martin H.D., Shears S.A., Johnson J.C., Smathers A.M., Palmer I.J. The endoscopic treatment of sciatic nerve entrapment/deep gluteal syndrome. Arthroscopy. 2011;27:172–181. - PubMed
-
- Byrd J.W.T., Polkowski G., Jones K.S. Endoscopic management of the snapping iliopsoas tendon. Arthroscopy. 2009;25:e18. (Abstr)
-
- Brown T. Thigh. In: Drez D.D., DeLee J.C., Miller M.D., editors. Vol 2. WB Saunders; Philadelphia: 2003. pp. 1481–1523. (Orthopaedic sports medicine: Principles and practice).
-
- Clanton T.O., Coupe K.J. Hamstring strains in athletes: Diagnosis and treatment. J Am Acad Orthop Surg. 1998;6:237–248. - PubMed
-
- Garrett W.E., Jr Muscle strain injuries. Am J Sports Med. 1996;24(Suppl):S2–S8. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
