A rare case of disseminated cysticercosis
- PMID: 23767025
- PMCID: PMC3680869
- DOI: 10.4103/2229-5070.105183
A rare case of disseminated cysticercosis
Abstract
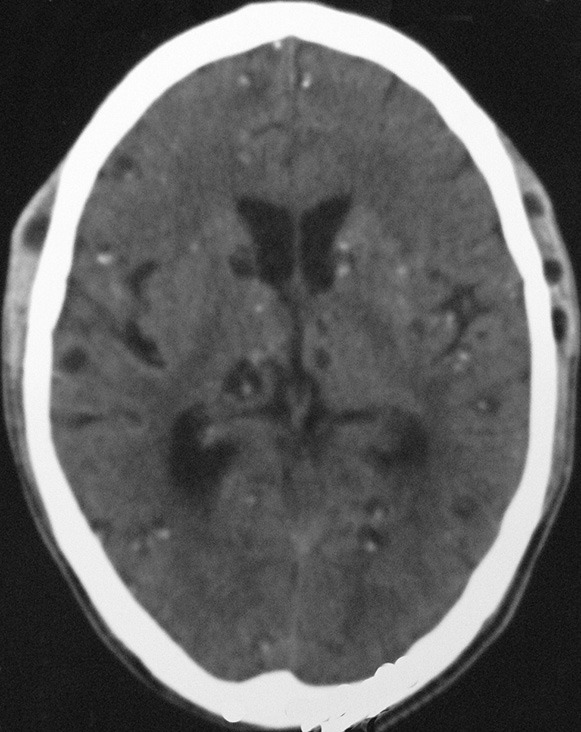
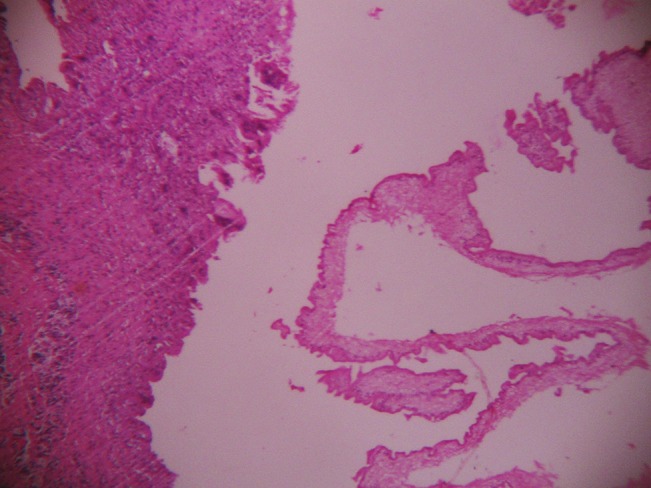
Cysticercosis is a common tropical disease. One of the uncommon manifestations and a rare complication is its disseminated form (DCC). Neurocysticercosis (NCC) is the common parasitic disease of the central nervous system. Human cysticercosis is caused by the dissemination of the embryo of Taenia solium in the intestine via the hepatoportal system to the tissues and organs of the body. The organs most commonly affected are the subcutaneous tissues, skeletal muscles, lungs, brain, eyes, liver, and occasionally the heart, thyroid, and pancreas. Widespread dissemination of the cysticerci can result in the involvement of almost any organ in the body. We report here a case of a 36-year-old-male with disseminated cysticercosis. He visited our hospital with symptoms of multiple palpable nodules, dementia, and confusion. After the investigations he was diagnosed with disseminated cysticercosis involving the brain, subcutaneous tissues all over the body, and the skeletal muscles. The patient was initially treated with Albendazole in a private hospital, but there was no response. Then he was treated with Praziquantel and steroids.
Keywords: Disseminated cysticercosis; Neurocysticercosis; cysticercosis.
Conflict of interest statement
Figures