

An in-silico comparison of proton beam and IMRT for postoperative radiotherapy in completely resected stage IIIA non-small cell lung cancer
- PMID: 23767810
- PMCID: PMC3695889
- DOI: 10.1186/1748-717X-8-144
An in-silico comparison of proton beam and IMRT for postoperative radiotherapy in completely resected stage IIIA non-small cell lung cancer
Abstract
Introduction: Post-operative radiotherapy (PORT) for stage IIIA completely-resected non-small cell lung cancer (CR-NSCLC) has been shown to improve local control; however, it is unclear that this translates into a survival benefit. One explanation is that the detrimental effect of PORT on critical organs at risk (OARs) negates its benefit. This study reports an in-silico comparative analysis of passive scattering proton therapy (PSPT)- and intensity modulated proton therapy (IMPT) with intensity modulated photon beam radiotherapy (IMRT) PORT.
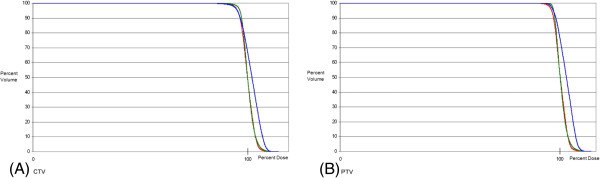
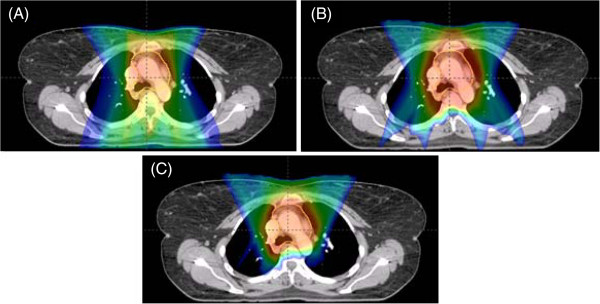
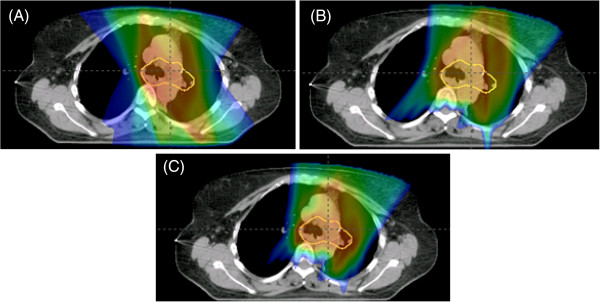
Methods: The computed tomography treatment planning scans of ten patients with pathologic stage IIIA CR-NSCLC treated with IMRT were used. IMRT, PSPT, and IMPT plans were generated and analyzed for dosimetric endpoints. The proton plans were constructed with two or three beams. All plans were optimized to deliver 50.4 Gy(RBE) in 1.8 Gy(RBE) fractions to the target volume.
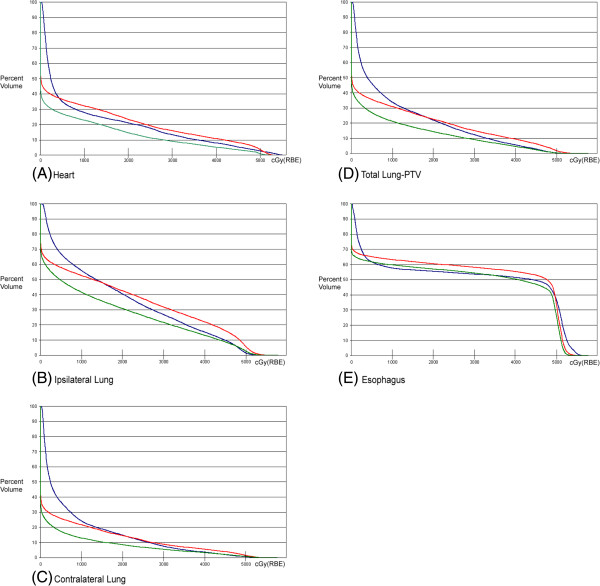
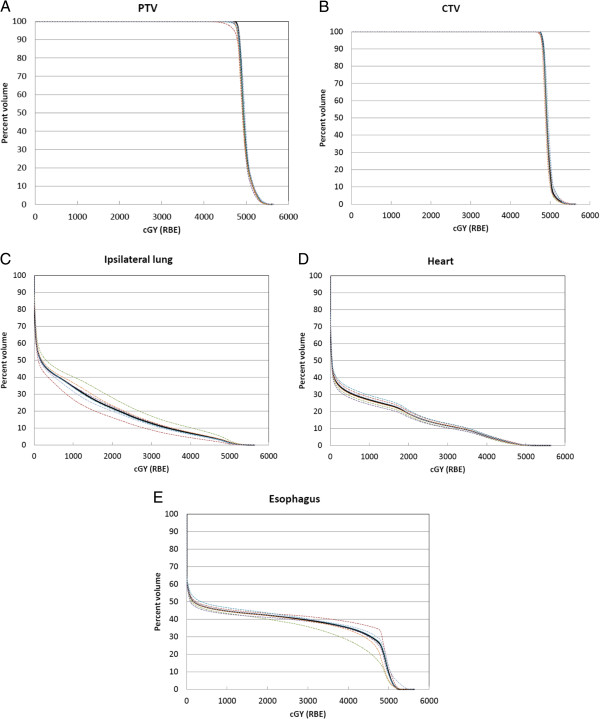
Results: IMPT leads to statistically significant reductions in maximum spinal cord, mean lung dose, lung volumes treated to 5, 10, 20, and 30 Gy (V5, V10, V20, V30), mean heart dose, and heart volume treated to 40 Gy (V40), when compared with IMRT or PSPT. PSPT reduced lung V5 but increased lung V20, V30, and heart and esophagus V40.
Conclusions: IMPT demonstrates a large decrease in dose to all OARs. PSPT, while reducing the low-dose lung bath, increases the volume of lung receiving high dose. Reductions are seen in dosimetric parameters predictive of radiation pneumonitis and cardiac morbidity and mortality. This reduction may correlate with a decrease in dose-limiting toxicity and improve the therapeutic ratio.
Figures
Similar articles
-
Intensity-modulated proton therapy reduces the dose to normal tissue compared with intensity-modulated radiation therapy or passive scattering proton therapy and enables individualized radical radiotherapy for extensive stage IIIB non-small-cell lung cancer: a virtual clinical study.Int J Radiat Oncol Biol Phys. 2010 Jun 1;77(2):357-66. doi: 10.1016/j.ijrobp.2009.04.028. Epub 2009 Aug 5. Int J Radiat Oncol Biol Phys. 2010. PMID: 19660879 Free PMC article.
-
Effects of respiratory motion on passively scattered proton therapy versus intensity modulated photon therapy for stage III lung cancer: are proton plans more sensitive to breathing motion?Int J Radiat Oncol Biol Phys. 2013 Nov 1;87(3):576-82. doi: 10.1016/j.ijrobp.2013.07.007. Int J Radiat Oncol Biol Phys. 2013. PMID: 24074932 Free PMC article. Clinical Trial.
-
Bayesian Adaptive Randomization Trial of Passive Scattering Proton Therapy and Intensity-Modulated Photon Radiotherapy for Locally Advanced Non-Small-Cell Lung Cancer.J Clin Oncol. 2018 Jun 20;36(18):1813-1822. doi: 10.1200/JCO.2017.74.0720. Epub 2018 Jan 2. J Clin Oncol. 2018. PMID: 29293386 Free PMC article. Clinical Trial.
-
Is there role of adjuvant radiotherapy after complete resection of locally advanced nonsmall cell lung cancer?Curr Opin Oncol. 2024 Jan 1;36(1):44-50. doi: 10.1097/CCO.0000000000001004. Epub 2023 Oct 20. Curr Opin Oncol. 2024. PMID: 37865829 Review.
-
Is there a role for arcing techniques in proton therapy?Br J Radiol. 2020 Mar 1;93(1107):20190469. doi: 10.1259/bjr.20190469. Epub 2020 Jan 3. Br J Radiol. 2020. PMID: 31860338 Free PMC article. Review.
Cited by
-
Trends in Postoperative Intensity-Modulated Radiation Therapy Use and Its Association With Survival Among Patients With Incompletely Resected Non-Small Cell Lung Cancer.JAMA Netw Open. 2022 Sep 1;5(9):e2230704. doi: 10.1001/jamanetworkopen.2022.30704. JAMA Netw Open. 2022. PMID: 36074462 Free PMC article.
-
Cardiac toxicity of lung cancer radiotherapy.Rep Pract Oncol Radiother. 2020 Jan-Feb;25(1):13-19. doi: 10.1016/j.rpor.2019.10.007. Epub 2019 Nov 14. Rep Pract Oncol Radiother. 2020. PMID: 31762693 Free PMC article. Review.
-
Dosimetric comparison of distal esophageal carcinoma plans for patients treated with small-spot intensity-modulated proton versus volumetric-modulated arc therapies.J Appl Clin Med Phys. 2019 Jul;20(7):15-27. doi: 10.1002/acm2.12623. Epub 2019 May 21. J Appl Clin Med Phys. 2019. PMID: 31112371 Free PMC article.
-
Comparison of proton therapy and intensity modulated photon radiotherapy for locally advanced non-small cell lung cancer: considerations for optimal trial design.J Thorac Dis. 2018 Apr;10(Suppl 9):S988-S990. doi: 10.21037/jtd.2018.04.59. J Thorac Dis. 2018. PMID: 29849214 Free PMC article. No abstract available.
-
Proton therapy for post-operative radiation therapy of non-small cell lung cancer.Transl Lung Cancer Res. 2018 Apr;7(2):205-209. doi: 10.21037/tlcr.2018.03.25. Transl Lung Cancer Res. 2018. PMID: 29876320 Free PMC article. Review.
References
-
- The Lung Cancer Study Group. Effects of postoperative mediastinal radiation on completely resected stage II and stage III epidermoid cancer of the lung. N Engl J Med. 1986;315(22):1377–1381. - PubMed
-
- PORT Meta-analysis Trialists Group. Postoperative radiotherapy in non-small-cell lung cancer: systematic review and meta-analysis of individual patient data from nine randomised controlled trials. Lancet. 1998;352(9124):257–263. - PubMed
-
- Miles EF, Kelsey CR, Kirkpatrick JP, Marks LB. Estimating the magnitude and field-size dependence of radiotherapy-induced mortality and tumor control after postoperative radiotherapy for non-small-cell lung cancer: calculations from clinical trials. Int J Radiat Oncol Biol Phys. 2007;68(4):1047–1052. doi: 10.1016/j.ijrobp.2007.02.028. - DOI - PubMed
-
- Douillard JY, Rosell R, De Lena M. et al.Impact of postoperative radiation therapy on survival in patients with complete resection and stage I, II, or IIIA non-small-cell lung cancer treated with adjuvant chemotherapy: the adjuvant Navelbine International Trialist Association (ANITA) Randomized Trial. Int J Radiat Oncol Biol Phys. 2008;72(3):695–701. doi: 10.1016/j.ijrobp.2008.01.044. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
