

CKD and cardiovascular disease in the Atherosclerosis Risk in Communities (ARIC) study: interactions with age, sex, and race
- PMID: 23769137
- PMCID: PMC3783539
- DOI: 10.1053/j.ajkd.2013.04.010
CKD and cardiovascular disease in the Atherosclerosis Risk in Communities (ARIC) study: interactions with age, sex, and race
Abstract
Background: Estimated glomerular filtration rate (eGFR) and albuminuria are central for diagnosis, staging, and risk evaluation in chronic kidney disease (CKD). Universal thresholds regardless of age, sex, and race are recommended, but relatively little is known about how these demographic factors alter the relationship of eGFR and albuminuria to cardiovascular outcomes.
Study design: Observational cohort study.
Setting & participants: 11,060 whites and blacks aged 52-75 years in the Atherosclerosis Risk in Communities (ARIC) Study with median follow-up of 11.2 years.
Predictors: eGFR by the CKD-EPI (CKD Epidemiology Collaboration) creatinine equation (reference, 95 mL/min/1.73 m(2)) and urinary albumin-creatinine ratio (ACR; reference, 5 mg/g).
Outcomes: Cardiovascular events (coronary disease, stroke, and heart failure) and all-cause mortality.
Measurements: Adjusted HRs associated with eGFR and ACR in subgroups according to age, sex, and race.
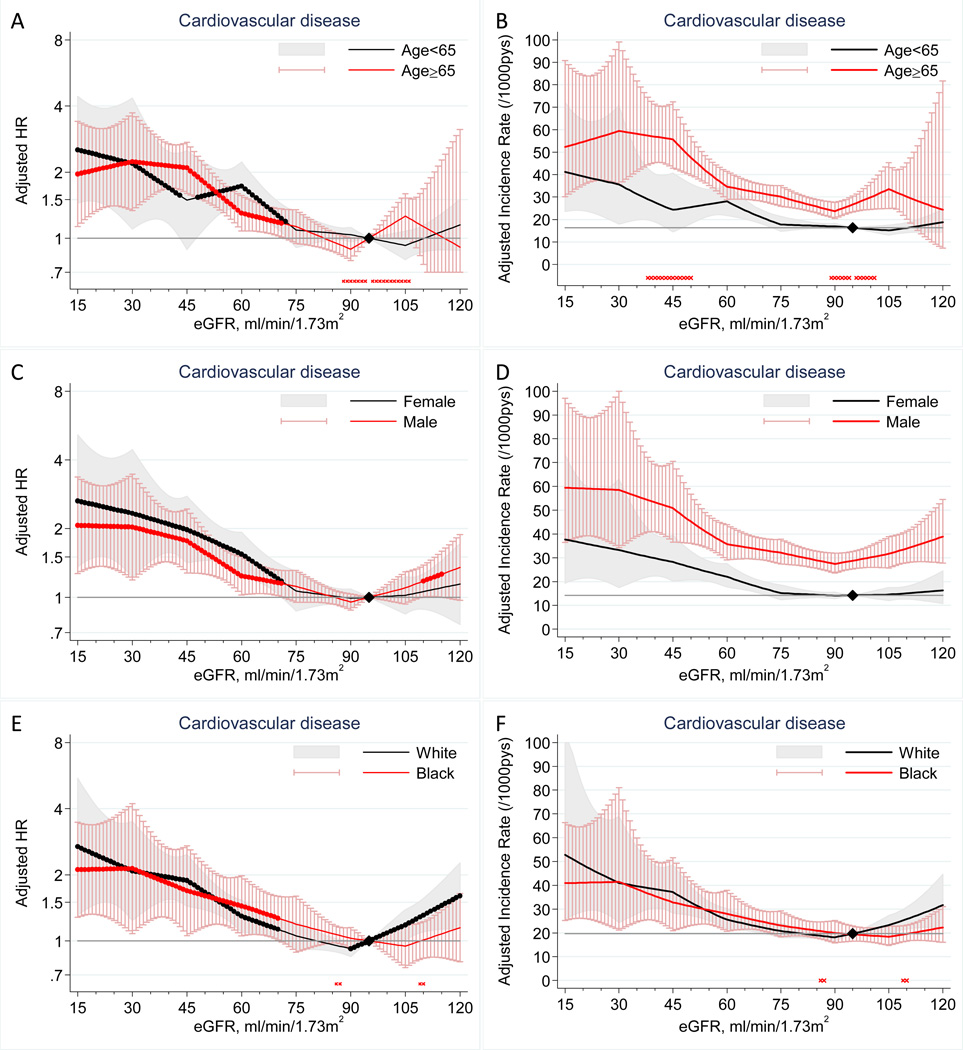
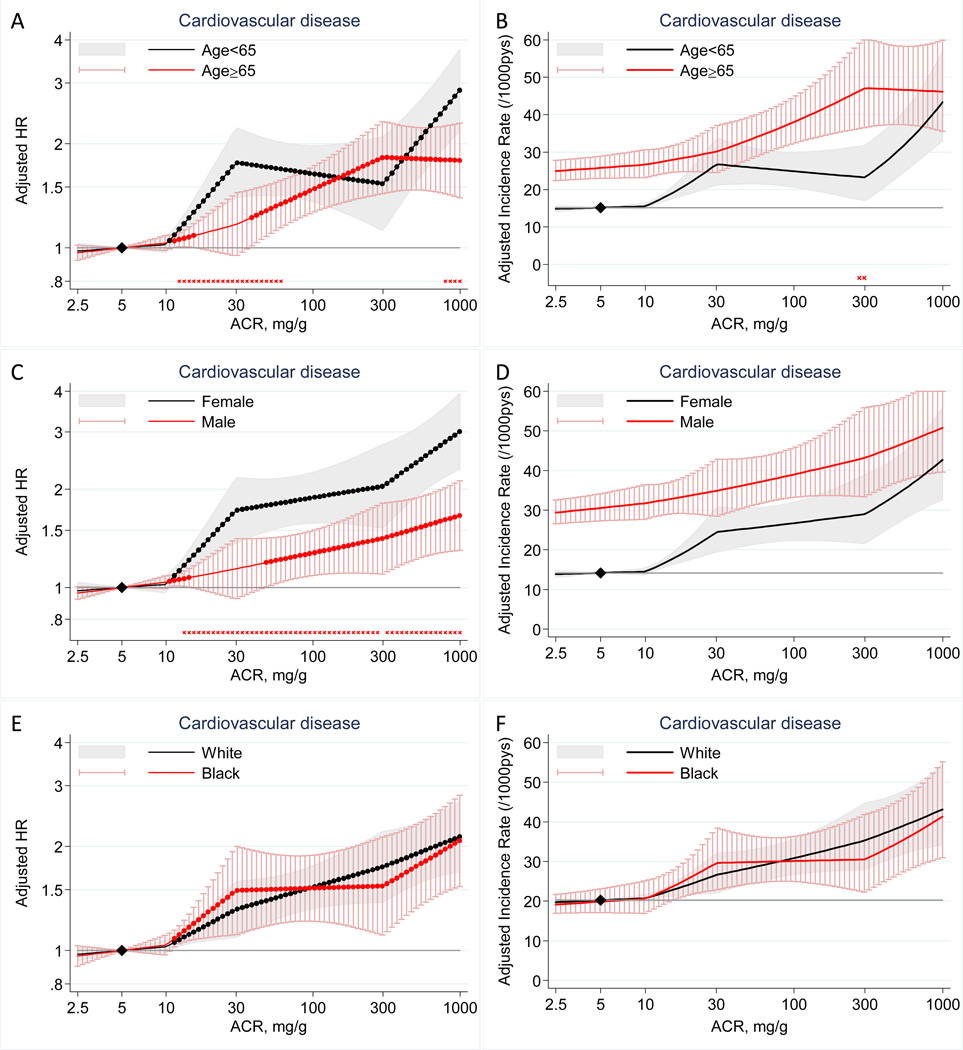
Results: Cardiovascular risk significantly increased at eGFR <70 mL/min/1.73 m(2) in all subgroups according to age (<65 vs ≥65 years), sex, and race (P for interaction >0.2 for these subgroups; eg, at eGFR of 30 mL/min/1.73 m(2), the adjusted HR was 2.19 [95% CI, 1.10-4.35] at age 52-64 years vs 2.23 [95% CI, 1.33-3.72] at age 65-75 years). Results were similar for mortality. Log(ACR) was associated linearly with cardiovascular risk without threshold effects in all subgroups, with some quantitative interactions. HRs according to ACR tended to be lower in men versus women (eg, at ACR of 40 mg/g, 1.18 [95% CI, 0.98-1.41] vs 1.77 [95% CI, 1.45-2.15]) and in the older versus younger population (1.24 [95% CI, 1.04-1.49] vs 1.73 [95% CI, 1.42-2.12]; P for interaction <0.01 for sex and age). Less evident interactions were observed for mortality.
Limitations: Single measurement of eGFR with creatinine and ACR and relatively narrow age range.
Conclusions: The associations of eGFR and ACR with cardiovascular events were largely similar, with some quantitative interactions, in age, sex, and racial subgroups, generally supporting universal thresholds of GFR and ACR for CKD definition/staging.
Keywords: Chronic kidney disease; all-cause mortality; cardiovascular disease; estimated glomerular filtration rate (eGFR); urinary albumin-creatinine ratio (ACR).
Copyright © 2013 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2013;(Suppl. 3)(1):1–150.
-
- Winearls CG, Glassock RJ. Dissecting and refining the staging of chronic kidney disease. Kidney Int. 2009 May;75(10):1009–1014. - PubMed
-
- IDF Clinical Guidelines Task Force. Global Guideline for Type 2 Diabetes. Brussels: International Diabetes Federation; 2012. - PubMed
-
- Barbour SJ, Er L, Djurdjev O, Karim M, Levin A. Differences in progression of CKD and mortality amongst Caucasian, Oriental Asian and South Asian CKD patients. Nephrol Dial Transplant. 2010 Nov 1;25(11):3663–3672. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- P30 DK079637/DK/NIDDK NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
