

Risk-standardizing survival for in-hospital cardiac arrest to facilitate hospital comparisons
- PMID: 23770167
- PMCID: PMC3769937
- DOI: 10.1016/j.jacc.2013.05.051
Risk-standardizing survival for in-hospital cardiac arrest to facilitate hospital comparisons
Abstract
Objectives: The purpose of this study is to develop a method for risk-standardizing hospital survival after cardiac arrest.
Background: A foundation with which hospitals can improve quality is to be able to benchmark their risk-adjusted performance against other hospitals, something that cannot currently be done for survival after in-hospital cardiac arrest.
Methods: Within the Get With The Guidelines (GWTG)-Resuscitation registry, we identified 48,841 patients admitted between 2007 and 2010 with an in-hospital cardiac arrest. Using hierarchical logistic regression, we derived and validated a model for survival to hospital discharge and calculated risk-standardized survival rates (RSSRs) for 272 hospitals with at least 10 cardiac arrest cases.
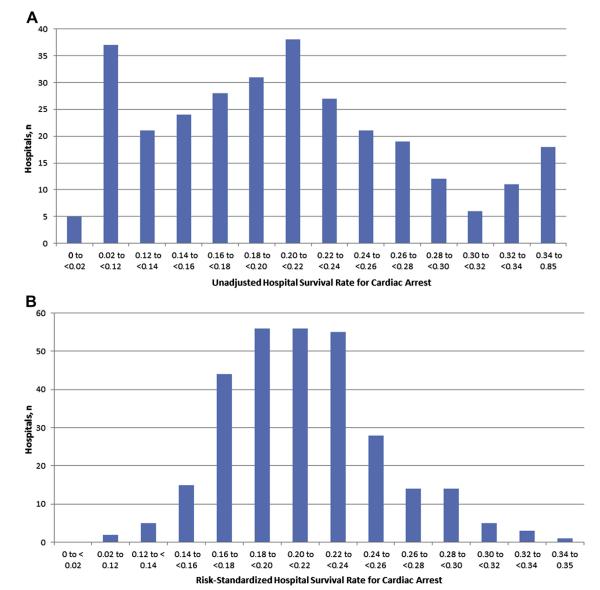
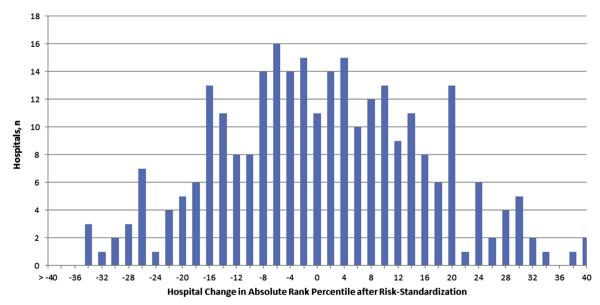
Results: The survival rate was 21.0% and 21.2% for the derivation and validation cohorts, respectively. The model had good discrimination (C-statistic 0.74) and excellent calibration. Eighteen variables were associated with survival to discharge, and a parsimonious model contained 9 variables with minimal change in model discrimination. Before risk adjustment, the median hospital survival rate was 20% (interquartile range: 14% to 26%), with a wide range (0% to 85%). After adjustment, the distribution of RSSRs was substantially narrower: median of 21% (interquartile range: 19% to 23%; range 11% to 35%). More than half (143 [52.6%]) of hospitals had at least a 10% positive or negative absolute change in percentile rank after risk standardization, and 50 (23.2%) had a ≥20% absolute change in percentile rank.
Conclusions: We have derived and validated a model to risk-standardize hospital rates of survival for in-hospital cardiac arrest. Use of this model can support efforts to compare hospitals in resuscitation outcomes as a foundation for quality assessment and improvement.
Keywords: AHA; American Heart Association; DNR; GWTG; Get With The Guidelines; cardiac arrest; do not resuscitate; risk adjustment; variation in care.
Copyright © 2013 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Chan PS, Nichol G, Krumholz HM, Spertus JA, Nallamothu BK. Hospital variation in time to defibrillation after in-hospital cardiac arrest. Arch Intern Med. 2009;169:1265–73. - PubMed
-
- Krumholz HM, Brindis RG, Brush JE, et al. Standards for statistical models used for public reporting of health outcomes: an American Heart Association Scientific Statement from the Quality of Care and Outcomes Research Interdisciplinary Writing Group. Circulation. 2006;113:456–62. - PubMed
-
- Krumholz HM, Wang Y, Mattera JA, et al. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with an acute myocardial infarction. Circulation. 2006;113:1683–92. - PubMed
-
- Krumholz HM, Wang Y, Mattera JA, et al. An administrative claims model suitable for profiling hospital performance based on 30-day mortality rates among patients with heart failure. Circulation. 2006;113:1693–701. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
