

A single center prospective study of bilateral breast reconstruction with free abdominal flaps: a critical analyses of 144 patients
- PMID: 23770544
- PMCID: PMC3692375
- DOI: 10.12659/MSM.883954
A single center prospective study of bilateral breast reconstruction with free abdominal flaps: a critical analyses of 144 patients
Abstract
Background: Bilateral breast reconstruction utilising autologous free tissue transfer is a complex procedure with multiple options for donor tissue available. Autogenous breast reconstruction techniques have evolved over the last three decades to meet this goal. The aim of this study was to determine the outcomes of patients undergoing bilateral breast reconstruction with DIEAP, TRAM or SIEA flaps.
Material and methods: A prospective study was performed in our Interdisciplinary Breast Centre from July 2004 until December 2011 in 144 patients. Demographic information, diabetes mellitus type I status, tobacco use, tumor stage, primary/secondary reconstruction, operative technique, adjuvant therapy received, length of follow-up, and complications were evaluated. Complications were divided into donor site and recipient site. To investigate which risk factors were independently related to flap loss (complete or partial), multiple linear regression analysis was performed.
Results: The study identified 144 patients who had bilateral breast reconstruction with DIEAP, TRAM or SIEA flaps. For all flaps (n=248), outcome included 98.4% survival and 0.7% vein microanastomosis revision. Recipient site complications included 1.6% complete flap loss, 0.8% fat necrosis, 2.9% partial skin loss/dehiscence flap necrosis and 2.0% haematoma rate. Donor site complications included 3.7% partial skin loss/dehiscence. There was evidence of abdominal bulges in TRAM patients (1.1%) but no hernias in any patients. BMI is a major determinant of flap loss (complete or partial) in these patients.
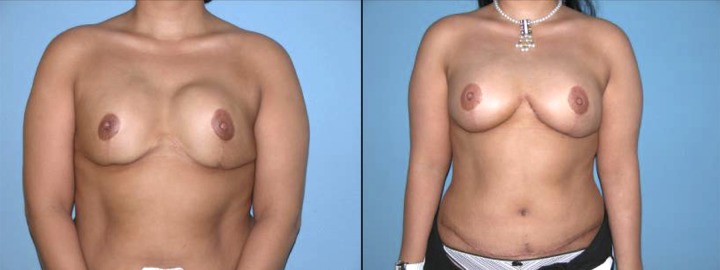
Conclusions: The primary goal of bilateral breast reconstruction is to provide a treatment option that can create a natural, symmetric breast mounds with minimal donor-site morbidity following bilateral mastectomies. These results support weight loss therapy prior to bilateral breast reconstruction.
Figures


References
-
- Al-Benna S, Steinstraesser L. Postablative reconstruction is better terminology than oncoplastic surgery. Plast Reconstr Surg. 2009;124:463e–64e. - PubMed
-
- Audretsch W, Andree C. Is mastectomy still justified – and if, in which patients? Onkologie. 2006;29:243–45. - PubMed
-
- Al-Benna S, Poggemann K, Steinau HU, Steinstraesser L. Diagnosis and Management of Primary Breast Sarcoma. Breast Cancer Res Treat. 2010;22(3):619–26. - PubMed
-
- Bach AD, Kneser U, Kopp J, Andree C, et al. Possibilities for breast reconstruction following cancer surgery. MMW Fortschr Med. 2004;146:40–42. 44. - PubMed
-
- Al-Benna Female plastic and reconstructive surgeons’ personal decision making for breast cancer treatment and reconstruction. Arch Gynecol Obstet. 2011;284:737–41. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
