

Real-time closed-loop control in a rodent model of medically induced coma using burst suppression
- PMID: 23770601
- PMCID: PMC3857134
- DOI: 10.1097/ALN.0b013e31829d4ab4
Real-time closed-loop control in a rodent model of medically induced coma using burst suppression
Abstract
Background: A medically induced coma is an anesthetic state of profound brain inactivation created to treat status epilepticus and to provide cerebral protection after traumatic brain injuries. The authors hypothesized that a closed-loop anesthetic delivery system could automatically and precisely control the electroencephalogram state of burst suppression and efficiently maintain a medically induced coma.
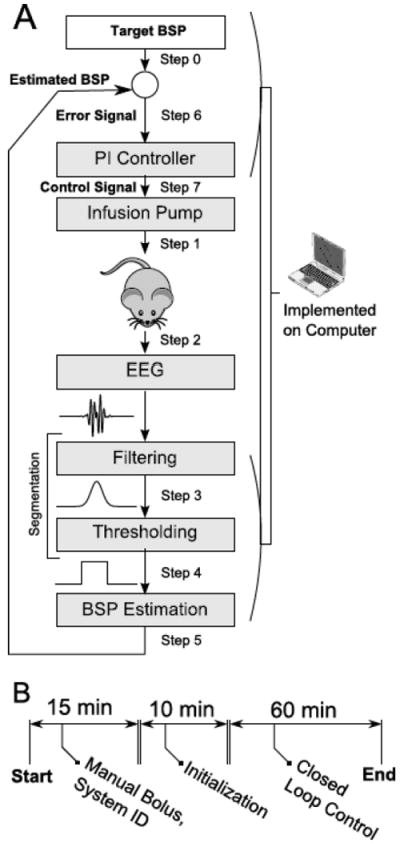
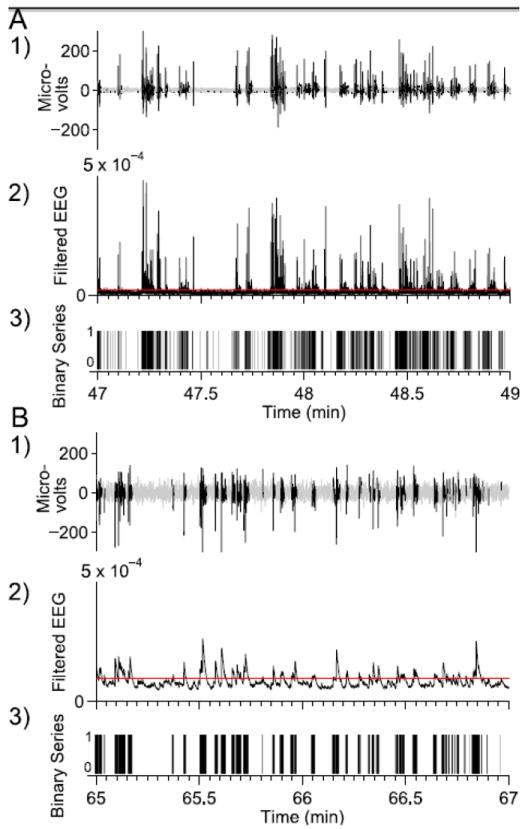
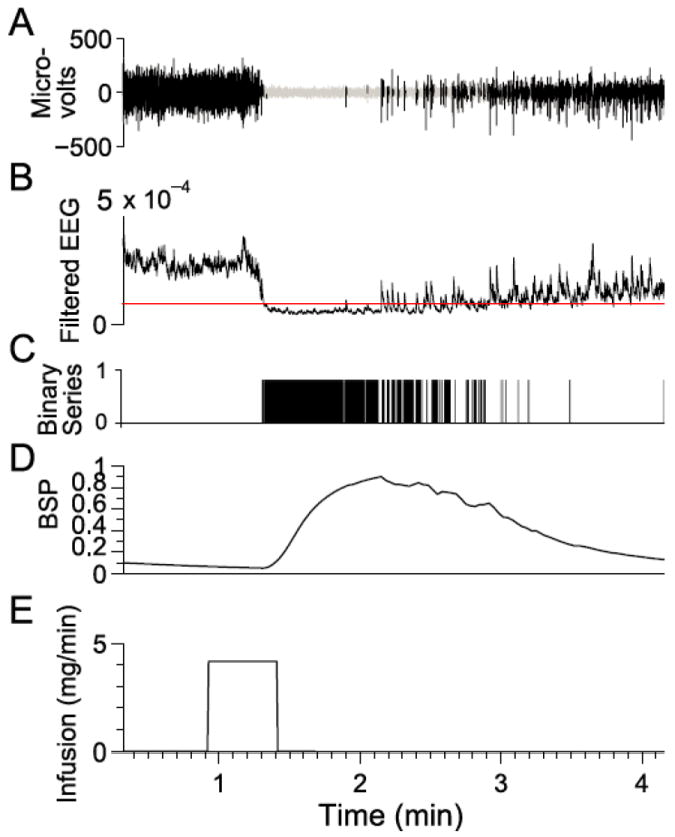
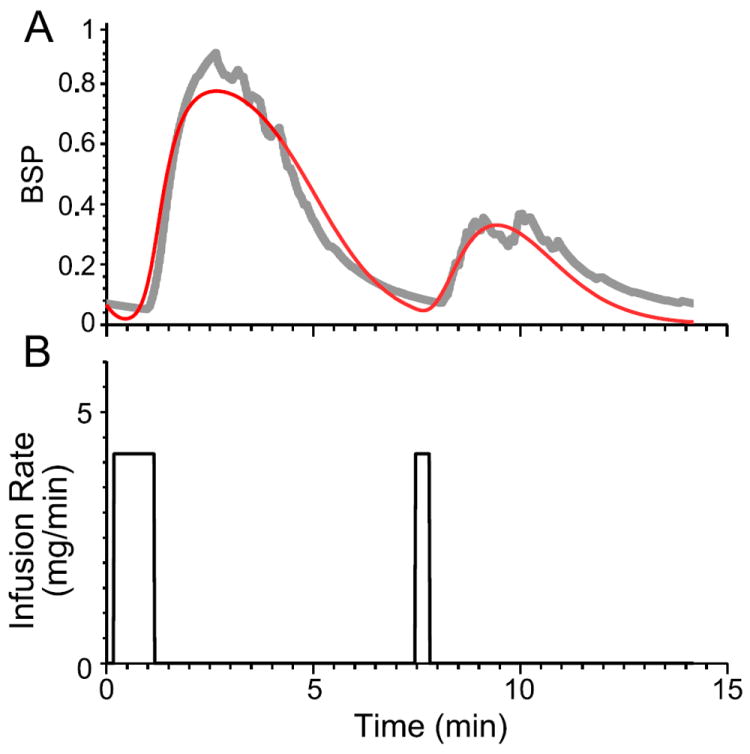
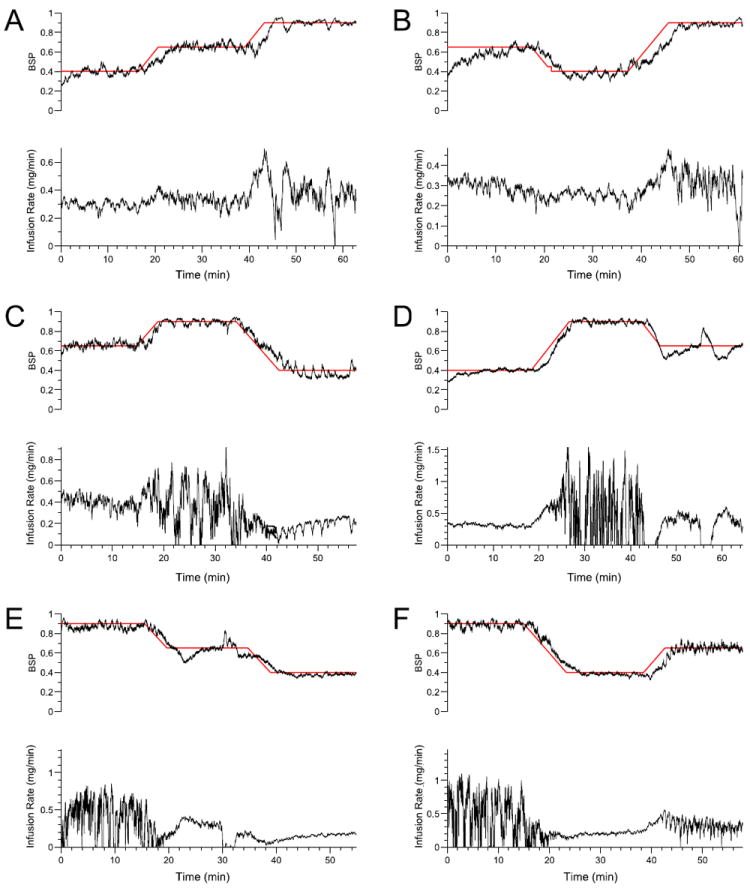
Methods: In six rats, the authors implemented a closed-loop anesthetic delivery system for propofol consisting of: a computer-controlled pump infusion, a two-compartment pharmacokinetics model defining propofol's electroencephalogram effects, the burst-suppression probability algorithm to compute in real time from the electroencephalogram the brain's burst-suppression state, an online parameter-estimation procedure and a proportional-integral controller. In the control experiment each rat was randomly assigned to one of the six burst-suppression probability target trajectories constructed by permuting the burst-suppression probability levels of 0.4, 0.65, and 0.9 with linear transitions between levels.
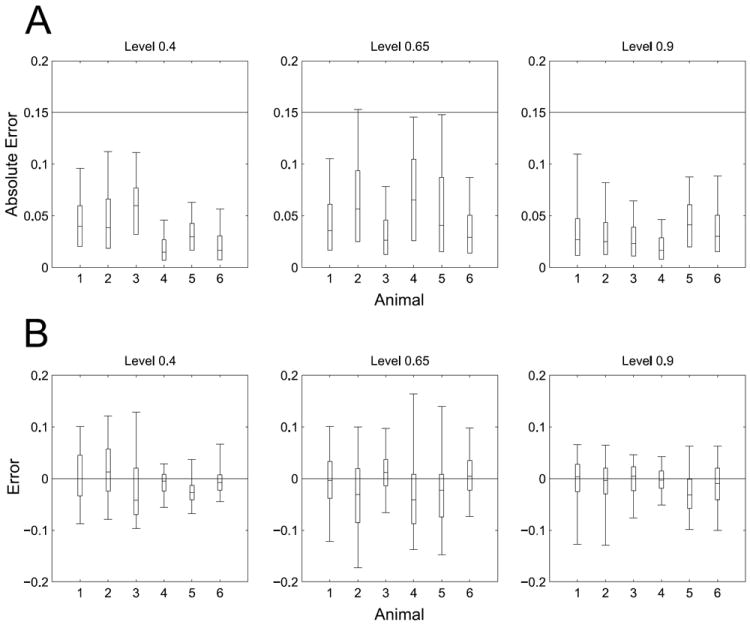
Results: In each animal the controller maintained approximately 60 min of tight, real-time control of burst suppression by tracking each burst-suppression probability target level for 15 min and two between-level transitions for 5-10 min. The posterior probability that the closed-loop anesthetic delivery system was reliable across all levels was 0.94 (95% CI, 0.77-1.00; n = 18) and that the system was accurate across all levels was 1.00 (95% CI, 0.84-1.00; n = 18).
Conclusion: The findings of this study establish the feasibility of using a closed-loop anesthetic delivery systems to achieve in real time reliable and accurate control of burst suppression in rodents and suggest a paradigm to precisely control medically induced coma in patients.
Conflict of interest statement
Figures
References
-
- Doyle PW, Matta BF. Burst suppression or isoelectric encephalogram for cerebral protection: Evidence from metabolic suppression studies. Can J Anaesth. 1999;57:725–35. - PubMed
-
- Rossetti AO, Logroscino G, Bromfield EB. Refractory status epilepticus: Effect of treatment aggressiveness on prognosis. Arch Neurol. 2005;62:1698–702. - PubMed
-
- Rossetti AO, Reichhart MD, Schaller MD, Despland PA, Bogousslavsky J. Propofol treatment of refractory status epilepticus: A study of 31 episodes. Epilepsia. 2004;45:757–63. - PubMed
-
- Amzica F. Basic physiology of burst-suppression. Epilepsia. 2009;50:38–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
