

Aortic dilation in bicuspid aortic valve disease: flow pattern is a major contributor and differs with valve fusion type
- PMID: 23771987
- PMCID: PMC3859916
- DOI: 10.1161/CIRCIMAGING.113.000528
Aortic dilation in bicuspid aortic valve disease: flow pattern is a major contributor and differs with valve fusion type
Abstract
Background: Ascending aortic dilation is important in bicuspid aortic valve (BAV) disease, with increased risk of aortic dissection. We used cardiovascular MR to understand the pathophysiology better by examining the links between 3-dimensional flow abnormalities, aortic function, and aortic dilation.
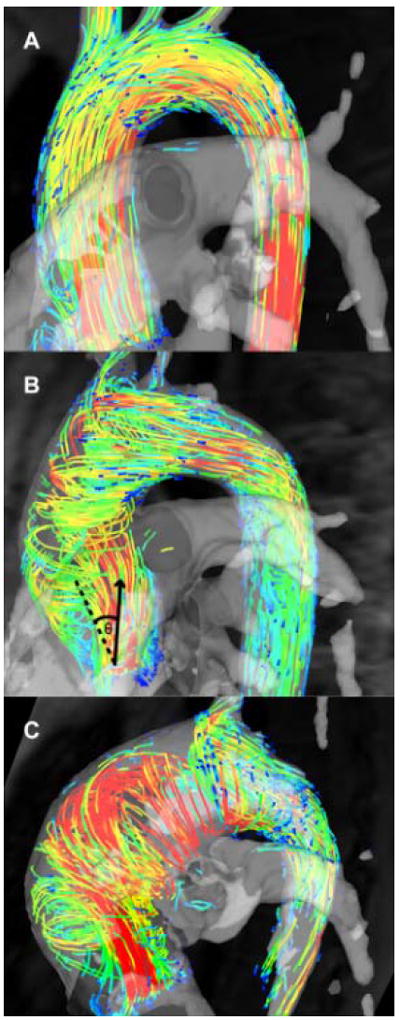
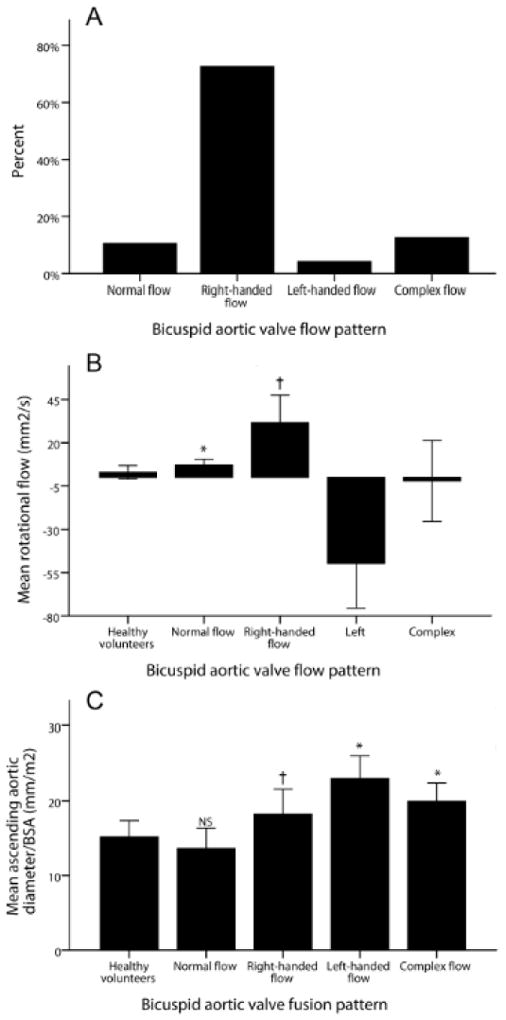
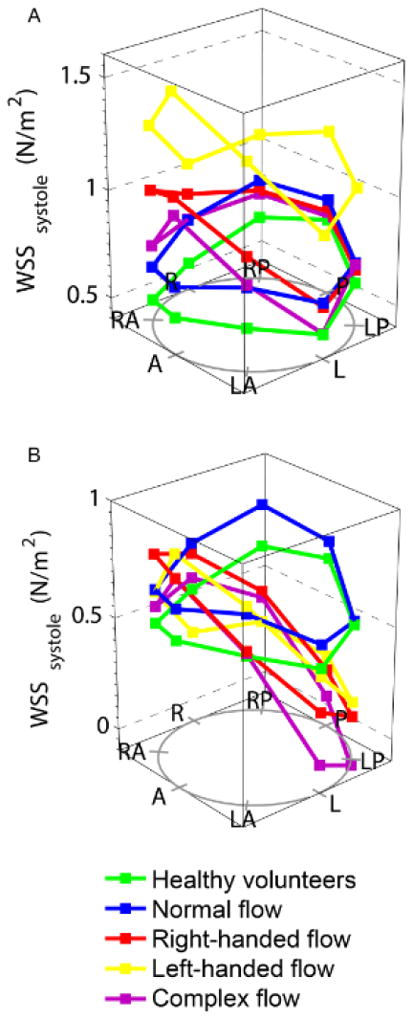
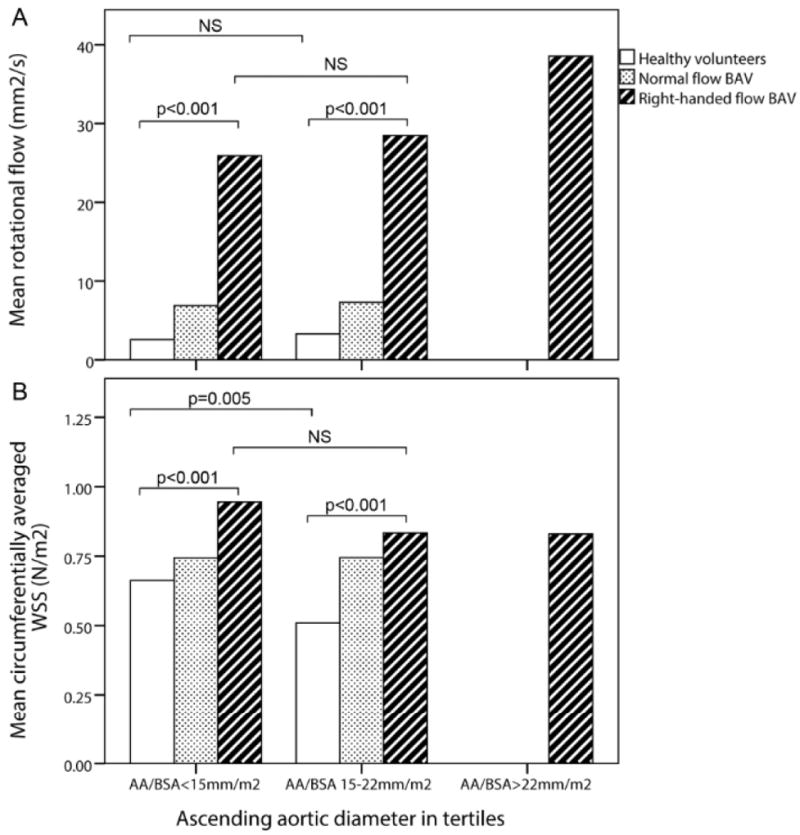
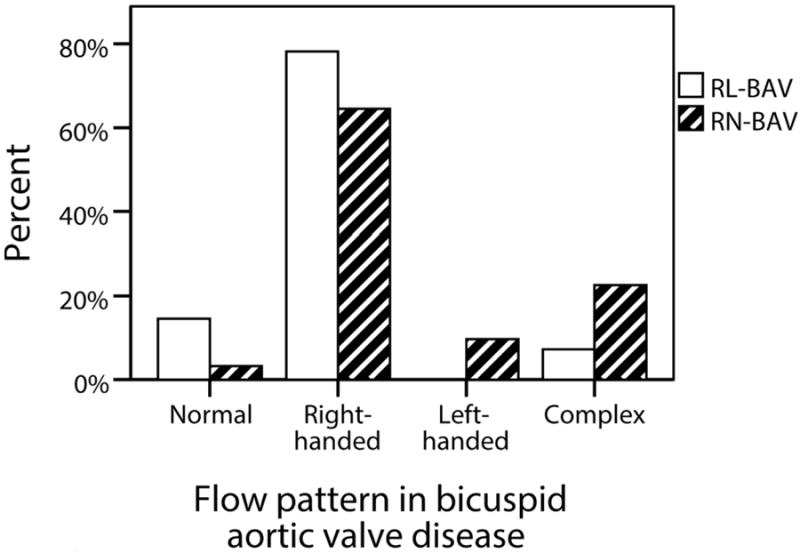
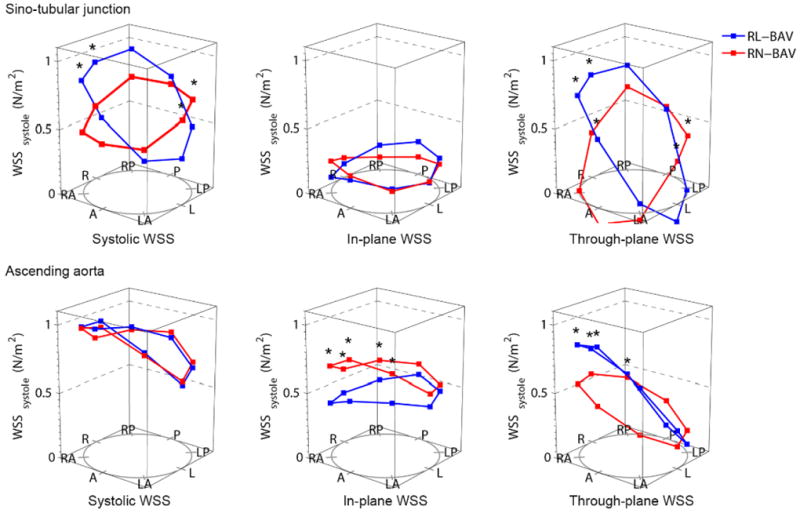
Methods and results: A total of 142 subjects underwent cardiovascular MR (mean age, 40 years; 95 with BAV, 47 healthy volunteers). Patients with BAV had predominantly abnormal right-handed helical flow in the ascending aorta, larger ascending aortas (18.3±3.3 versus 15.2±2.2 mm/m²; P<0.001), and higher rotational (helical) flow (31.7±15.8 versus 2.9±3.9 mm²/s; P<0.001), systolic flow angle (23.1°±12.5° versus 7.0°±4.6°; P<0.001), and systolic wall shear stress (0.85±0.28 versus 0.59±0.17 N/m²; P<0.001) compared with healthy volunteers. BAV with right-handed flow and right-non coronary cusp fusion (n=31) showed more severe flow abnormalities (rotational flow, 38.5±16.5 versus 27.8±12.4 mm²/s; P<0.001; systolic flow angle, 29.4°±10.9° versus 19.4°±11.4°; P<0.001; in-plane wall shear stress, 0.64±0.23 versus 0.47±0.22 N/m²; P<0.001) and larger aortas (19.5±3.4 versus 17.5±3.1 mm/m²; P<0.05) than right-left cusp fusion (n=55). Patients with BAV with normal flow patterns had similar aortic dimensions and wall shear stress to healthy volunteers and younger patients with BAV showed abnormal flow patterns but no aortic dilation, both further supporting the importance of flow pattern in the pathogenesis of aortic dilation. Aortic function measures (distensibility, aortic strain, and pulse wave velocity) were similar across all groups.
Conclusions: Flow abnormalities may be a major contributor to aortic dilation in BAV. Fusion type affects the severity of flow abnormalities and may allow better risk prediction and selection of patients for earlier surgical intervention.
Keywords: aorta; bicuspid aortic valve; cardiac MRI; vascular function; wall shear stress.
Figures
Comment in
-
Letter by Girdauskas regarding article, "Aortic dilation in bicuspid aortic valve disease: flow pattern is a major contributor and differs with valve fusion type".Circ Cardiovasc Imaging. 2014 Jan;7(1):213. doi: 10.1161/CIRCIMAGING.113.001476. Circ Cardiovasc Imaging. 2014. PMID: 24449555 No abstract available.
-
Response to letter regarding article, "Aortic dilation in bicuspid aortic valve disease: flow pattern is a major contributor and differs with valve fusion type".Circ Cardiovasc Imaging. 2014 Jan;7(1):214. doi: 10.1161/CIRCIMAGING.113.001497. Circ Cardiovasc Imaging. 2014. PMID: 24449556 Free PMC article. No abstract available.
References
-
- Sievers HH, Sievers HL. Aortopathy in bicuspid aortic valve disease - genes or hemodynamics? or Scylla and Charybdis? Eur J Cardiothorac Surg. 2011;39:803–804. - PubMed
-
- Loscalzo ML, Goh DL, Loeys B, Kent KC, Spevak PJ, Dietz HC. Familial thoracic aortic dilation and bicommissural aortic valve: a prospective analysis of natural history and inheritance. Am J Med Genet A. 2007;143A:1960–1967. - PubMed
-
- Girdauskas E, Borger MA, Secknus MA, Girdauskas G, Kuntze T. Is aortopathy in bicuspid aortic valve disease a congenital defect or a result of abnormal hemodynamics? A critical reappraisal of a one-sided argument. Eur J Cardiothorac Surg. 2011;39:809–814. - PubMed
-
- Fernandez B, Duran AC, Fernandez-Gallego T, Fernandez MC, Such M, Arque JM, Sans-Coma V. Bicuspid aortic valves with different spatial orientations of the leaflets are distinct etiological entities. J Am Coll Cardiol. 2009;54:2312–2318. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
