

Pathobiology of HIV/SIV-associated changes in secondary lymphoid tissues
- PMID: 23772615
- PMCID: PMC6066369
- DOI: 10.1111/imr.12070
Pathobiology of HIV/SIV-associated changes in secondary lymphoid tissues
Abstract
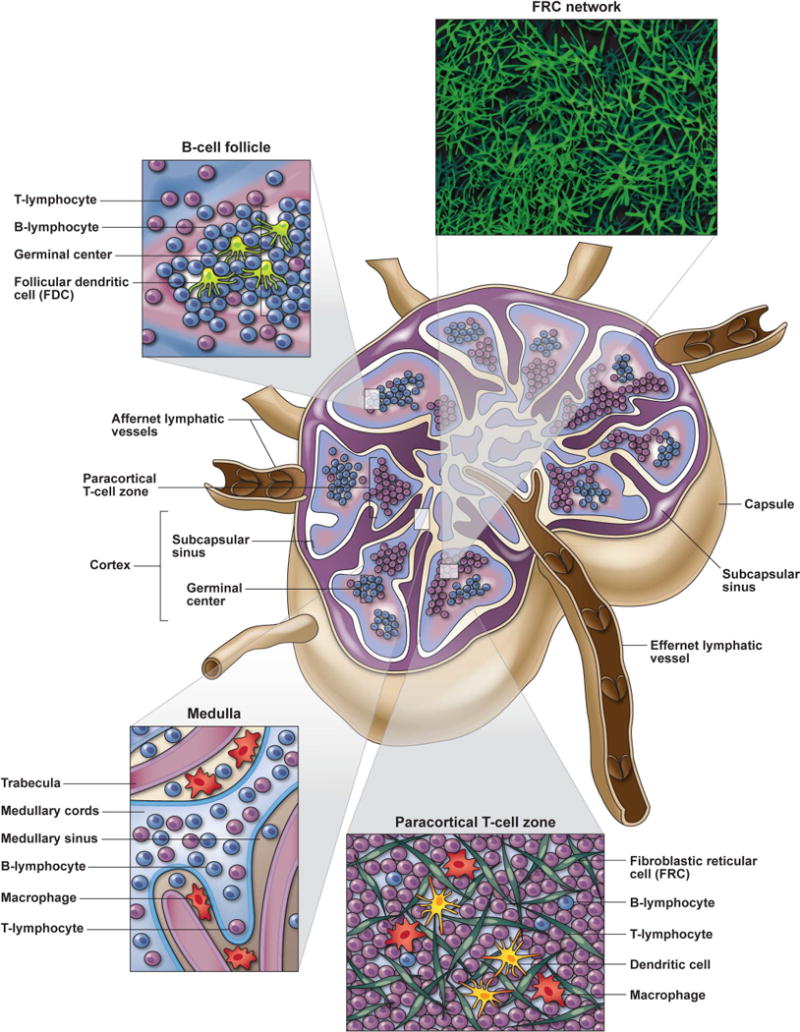
Acquired immunodeficiency syndrome (AIDS) is principally a disease of lymphoid tissues (LTs), due to the fact that the main target cell of human immunodeficiency virus (HIV) is the CD4(+) T lymphocyte that primarily resides within organs of the immune system. The impact of HIV infection on secondary LTs, in particular lymph nodes, is critical to delineate, as these immune organs are the principal sites for initiating and facilitating immune responses and are critical for lymphocyte homeostatic maintenance and survival. The underlying structural elements of LTs, fibroblastic reticular cell (FRC) network, not only form the architectural framework for these organs, but also play in integral role in the production and storage of cytokines needed for T-cell survival. There is an interdependent relationship between the FRC stromal network and CD4(+) T lymphocytes for their survival and maintenance that is progressively disrupted during HIV disease. HIV infection results in profound pathological changes to LTs induced by persistent chronic immune activation and inflammation that leads to progressive collagen deposition and fibrosis disrupting and damaging the important FRC network. In this review, I focus on the process, mechanisms, and the implications of pathological damage to important secondary LTs, combining what we have learned from HIV-infected individuals as well as the invaluable knowledge gained from studies in non-human primate simian immunodeficiency virus infection models.
Published 2013. This article is a U.S. Government work and is in the public domain in the USA.
Figures

References
-
- Trepel F. Number and distribution of lymphocytes in man. A critical analysis. Klin Wochenschr. 1974;52:511–515. - PubMed
-
- Butcher EC, Picker LJ. Lymphocyte homing and homeostasis. Science. 1996;272:60–66. - PubMed
-
- Willard-Mack CL. Normal structure, function, and histology of lymph nodes. Toxicol Pathol. 2006;34:409–424. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
