

The relationship between anisometropia and amblyopia
- PMID: 23773832
- PMCID: PMC3773531
- DOI: 10.1016/j.preteyeres.2013.05.001
The relationship between anisometropia and amblyopia
Abstract
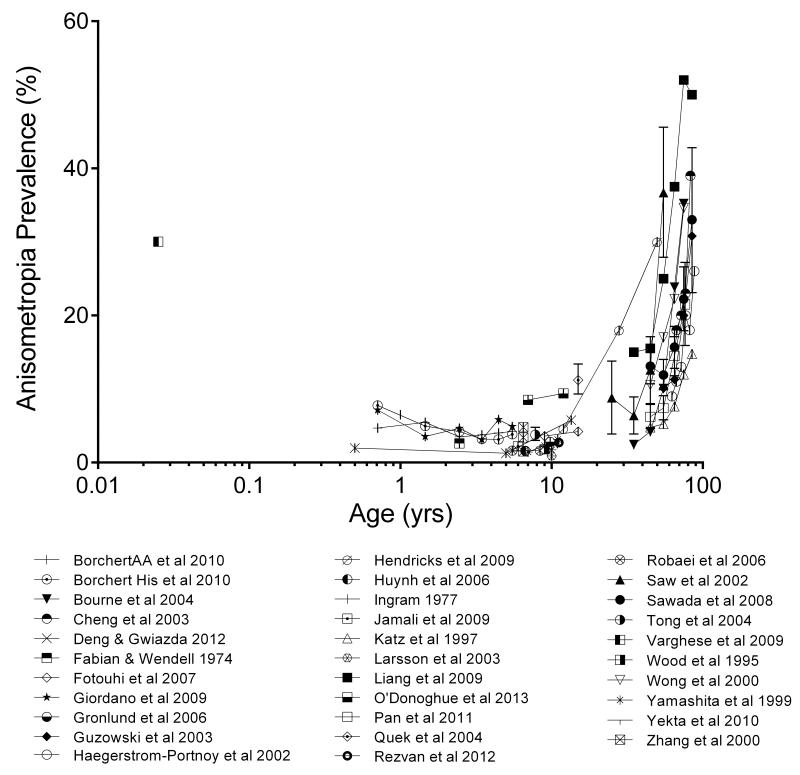
This review aims to disentangle cause and effect in the relationship between anisometropia and amblyopia. Specifically, we examine the literature for evidence to support different possible developmental sequences that could ultimately lead to the presentation of both conditions. The prevalence of anisometropia is around 20% for an inter-ocular difference of 0.5D or greater in spherical equivalent refraction, falling to 2-3%, for an inter-ocular difference of 3D or above. Anisometropia prevalence is relatively high in the weeks following birth, in the teenage years coinciding with the onset of myopia and, most notably, in older adults starting after the onset of presbyopia. It has about one-third the prevalence of bilateral refractive errors of the same magnitude. Importantly, the prevalence of anisometropia is higher in highly ametropic groups, suggesting that emmetropization failures underlying ametropia and anisometropia may be similar. Amblyopia is present in 1-3% of humans and around one-half to two-thirds of amblyopes have anisometropia either alone or in combination with strabismus. The frequent co-existence of amblyopia and anisometropia at a child's first clinical examination promotes the belief that the anisometropia has caused the amblyopia, as has been demonstrated in animal models of the condition. In reviewing the human and monkey literature however it is clear that there are additional paths beyond this classic hypothesis to the co-occurrence of anisometropia and amblyopia. For example, after the emergence of amblyopia secondary to either deprivation or strabismus, anisometropia often follows. In cases of anisometropia with no apparent deprivation or strabismus, questions remain about the failure of the emmetropization mechanism that routinely eliminates infantile anisometropia. Also, the chronology of amblyopia development is poorly documented in cases of 'pure' anisometropic amblyopia. Although indirect, the therapeutic impact of refractive correction on anisometropic amblyopia provides strong support for the hypothesis that the anisometropia caused the amblyopia. Direct evidence for the aetiology of anisometropic amblyopia will require longitudinal tracking of at-risk infants, which poses numerous methodological and ethical challenges. However, if we are to prevent this condition, we must understand the factors that cause it to develop.
Keywords: Amblyopia; Anisometropia; Anisometropic amblyopia; Emmetropization; Refractive error; Visual development.
Crown Copyright © 2013. Published by Elsevier Ltd. All rights reserved.
Figures





References
-
- Abrahamsson M, Fabian G, Andersson AK, Sjostrand J. A longitudinal study of a population based sample of astigmatic children. I. Refraction and amblyopia. Acta Ophthalmologica. 1990a;68(4):428–434. - PubMed
-
- Abrahamsson M, Fabian G, Sjostrand J. A longitudinal study of a population based sample of astigmatic children. II. The changeability of anisometropia. Acta Ophthalmologica. 1990b;68(4):435–440. - PubMed
-
- Adams RJ, Dalton SM, Murphy AM, Hall HL, Courage ML. Testing young infants with the Welch Allyn suresight non-cycloplegic autorefractor. Ophthalmic & Physiological Optics. 2002;22(6):546–551. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
