

Caveats for the use of operational electronic health record data in comparative effectiveness research
- PMID: 23774517
- PMCID: PMC3748381
- DOI: 10.1097/MLR.0b013e31829b1dbd
Caveats for the use of operational electronic health record data in comparative effectiveness research
Abstract
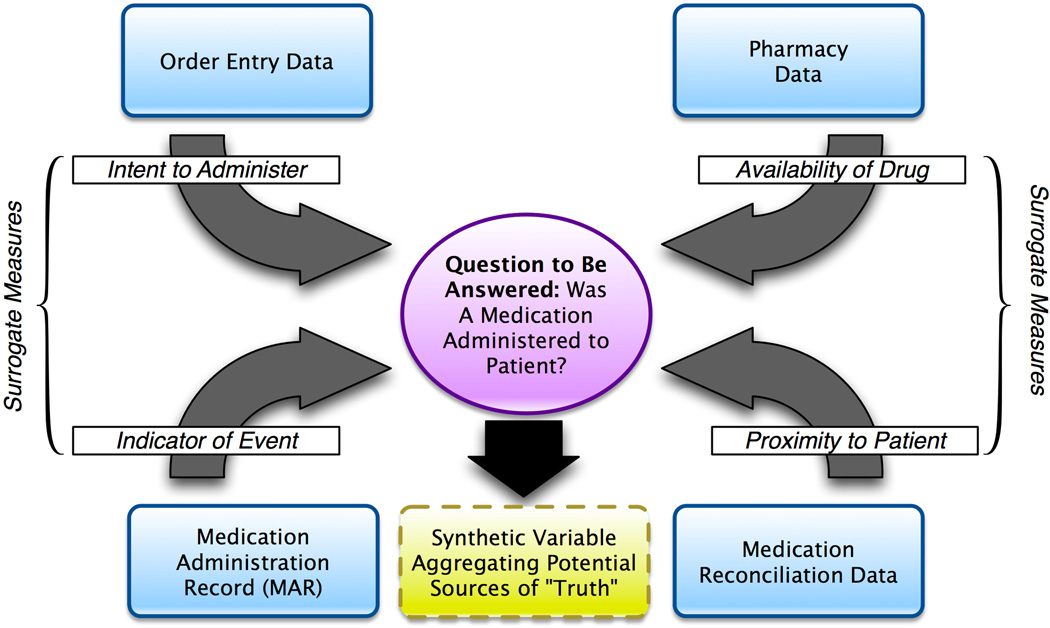
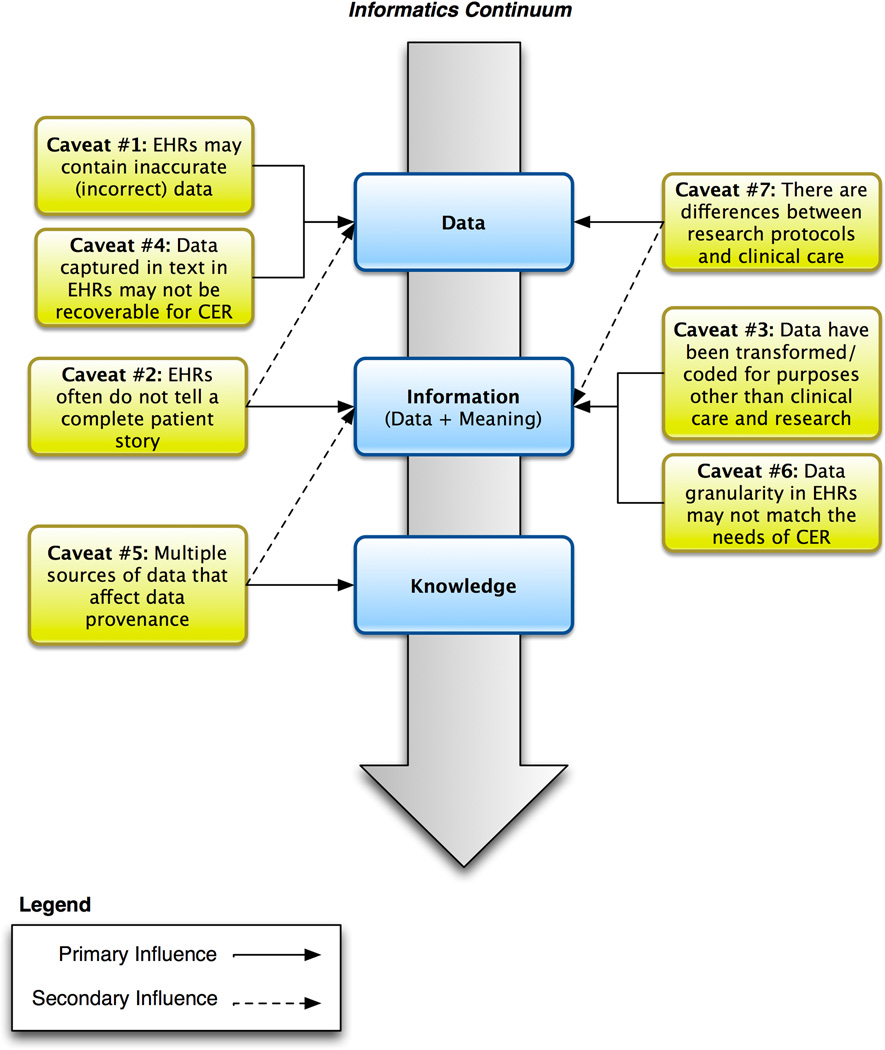
The growing amount of data in operational electronic health record systems provides unprecedented opportunity for its reuse for many tasks, including comparative effectiveness research. However, there are many caveats to the use of such data. Electronic health record data from clinical settings may be inaccurate, incomplete, transformed in ways that undermine their meaning, unrecoverable for research, of unknown provenance, of insufficient granularity, and incompatible with research protocols. However, the quantity and real-world nature of these data provide impetus for their use, and we develop a list of caveats to inform would-be users of such data as well as provide an informatics roadmap that aims to insure this opportunity to augment comparative effectiveness research can be best leveraged.
Figures
References
-
- Blumenthal D, Tavenner M. The “meaningful use” regulation for electronic health records. New England Journal of Medicine. 2010;363:501–504. - PubMed
-
- Weiner MG, Embi PJ. Toward reuse of clinical data for research and quality improvement: the end of the beginning. Annals of Internal Medicine. 2009;151:359–360. - PubMed
-
- Friedman CP, Wong AK, Blumenthal D. Achieving a nationwide learning health system. Science Translational Medicine. 2010;2(57):57cm29. http://stm.sciencemag.org/content/2/57/57cm29.full. - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR000090/TR/NCATS NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- 8UL1TR000090/TR/NCATS NIH HHS/United States
- 1UL1RR024148/RR/NCRR NIH HHS/United States
- UL1 RR024156/RR/NCRR NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- UL1 RR024148/RR/NCRR NIH HHS/United States
- 5UL1RR025008/RR/NCRR NIH HHS/United States
- UL1 RR024140/RR/NCRR NIH HHS/United States
- UL1 RR025008/RR/NCRR NIH HHS/United States
- 5UL1RR025005/RR/NCRR NIH HHS/United States
- 2UL1RR024156/RR/NCRR NIH HHS/United States
- 5UL1RR024140/RR/NCRR NIH HHS/United States
