

Diet and physical activity for the prevention of noncommunicable diseases in low- and middle-income countries: a systematic policy review
- PMID: 23776415
- PMCID: PMC3679005
- DOI: 10.1371/journal.pmed.1001465
Diet and physical activity for the prevention of noncommunicable diseases in low- and middle-income countries: a systematic policy review
Abstract
Background: Diet-related noncommunicable diseases (NCDs) are increasing rapidly in low- and middle-income countries (LMICs) and constitute a leading cause of mortality. Although a call for global action has been resonating for years, the progress in national policy development in LMICs has not been assessed. This review of strategies to prevent NCDs in LMICs provides a benchmark against which policy response can be tracked over time.
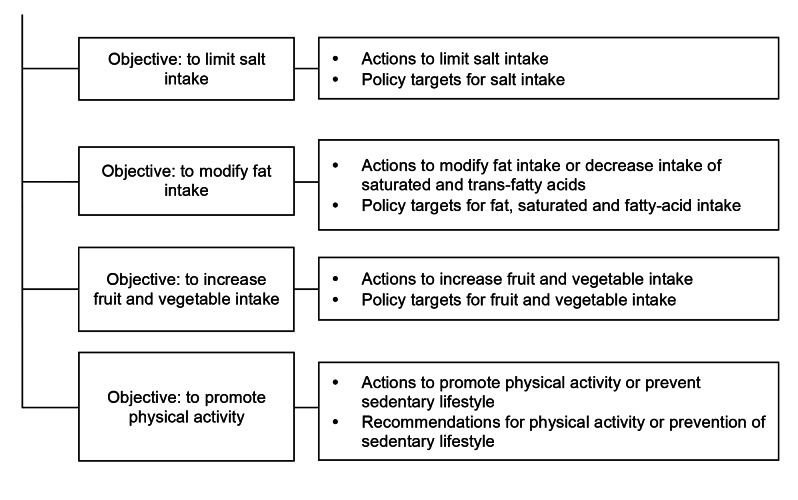
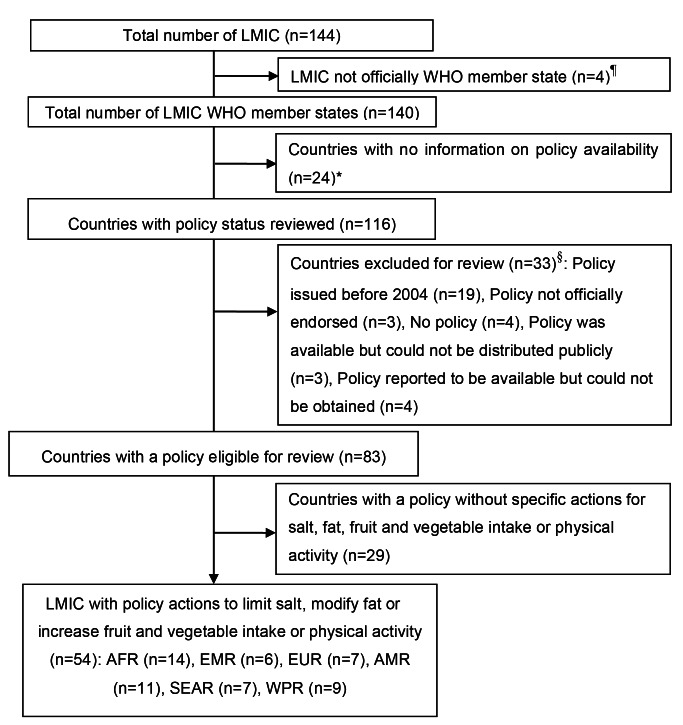
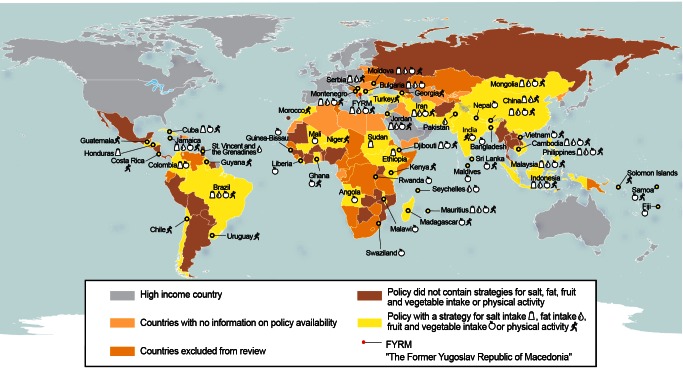
Methods and findings: We reviewed how government policies in LMICs outline actions that address salt consumption, fat consumption, fruit and vegetable intake, or physical activity. A structured content analysis of national nutrition, NCDs, and health policies published between 1 January 2004 and 1 January 2013 by 140 LMIC members of the World Health Organization (WHO) was carried out. We assessed availability of policies in 83% (116/140) of the countries. NCD strategies were found in 47% (54/116) of LMICs reviewed, but only a minority proposed actions to promote healthier diets and physical activity. The coverage of policies that specifically targeted at least one of the risk factors reviewed was lower in Africa, Europe, the Americas, and the Eastern Mediterranean compared to the other two World Health Organization regions, South-East Asia and Western Pacific. Of the countries reviewed, only 12% (14/116) proposed a policy that addressed all four risk factors, and 25% (29/116) addressed only one of the risk factors reviewed. Strategies targeting the private sector were less frequently encountered than strategies targeting the general public or policy makers.
Conclusions: This review indicates the disconnection between the burden of NCDs and national policy responses in LMICs. Policy makers urgently need to develop comprehensive and multi-stakeholder policies to improve dietary quality and physical activity.
Conflict of interest statement
The authors have declared that no competing interests exist. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the views, decisions, or policies of the institutions with which they are affiliated.
Figures
Comment in
-
Malignant neglect: the failure to address the need to prevent premature non-communicable disease morbidity and mortality.PLoS Med. 2013;10(6):e1001466. doi: 10.1371/journal.pmed.1001466. Epub 2013 Jun 11. PLoS Med. 2013. PMID: 23776416 Free PMC article.
-
Addressing the wicked problem of obesity through planning and policies.PLoS Med. 2013;10(6):e1001475. doi: 10.1371/journal.pmed.1001475. Epub 2013 Jun 25. PLoS Med. 2013. PMID: 23824681 Free PMC article.
References
-
- World Health Organization (2011) Global status report on noncommunicable diseases. Geneva: World Health Organization.
-
- Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K (2007) Chronic diseases 1—the burden and costs of chronic diseases in low-income and middle-income countries. Lancet 370: 1929–1938 ISI:000251517600031. - PubMed
-
- Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, et al.. (2011) The global economic burden of noncommunicable diseases. Geneva: World Economic Forum. 48 p.
-
- Cecchini M, Sassi F, Lauer JA, Lee YY, Guajardo-Barron V, et al. (2010) Tackling of unhealthy diets, physical inactivity, and obesity: health effects and cost-effectiveness. Lancet 376: 1775–1784 ISI:000284984900033. - PubMed
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, et al. (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380: 2224–2260. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
