Thyroid ultrasound
- PMID: 23776892
- PMCID: PMC3683194
- DOI: 10.4103/2230-8210.109667
Thyroid ultrasound
Abstract
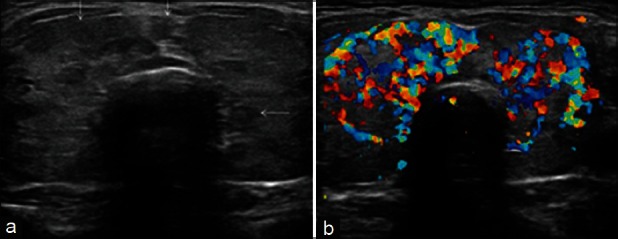
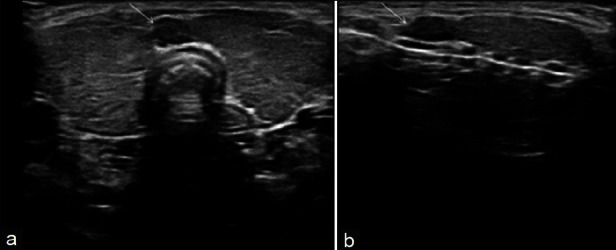
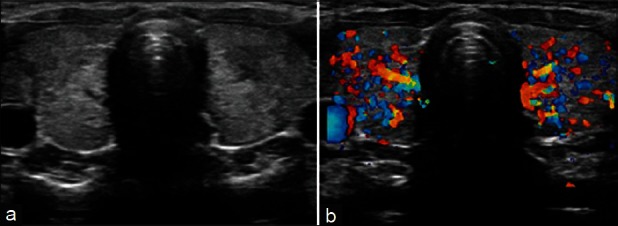
Thyroid ultrasonography has established itself as a popular and useful tool in the evaluation and management of thyroid disorders. Advanced ultrasound techniques in thyroid imaging have not only fascinated the radiologists but also attracted the surgeons and endocrinologists who are using these techniques in their daily clinical and operative practice. This review provides an overview of indications for ultrasound in various thyroid diseases, describes characteristic ultrasound findings in these diseases, and illustrates major diagnostic pitfalls of thyroid ultrasound.
Keywords: Color doppler; high resolution ultrasonography; thyroid; ultrasound; ultrasound elastography.
Conflict of interest statement
Figures
References
-
- Solbiati L, Charboneau JW, Osti V, James EM, Hay ID. The thyroid gland. In: Rumack CM, Wilson SR, Charboneau JW, editors. Diagnostic Ultrasound. 3rd ed. Vol. 1. St. Louis, Missouri: Elsevier Mosby; 2005. pp. 735–70.
-
- Gharib H, Papini E, Valcavi R, Baskin HJ, Crescenzi A, Dottorini ME, et al. American Association of Clinical Endocrinologists and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocr Pract. 2006;12:63–102. - PubMed
-
- Baskin HJ. Ultrasound of thyroid nodules. In: Baskin HJ, editor. Thyroid Ultrasound and Ultrasound-guided FNA Biopsy. Boston: Kluwer Academic Publisher; 2007. pp. 71–86.
-
- Moon WJ, Jung SL, Lee JH, Na DG, Baek JH, Lee YH, et al. Benign and malignant thyroid nodules: US differentiation–multicenter retrospective study. Radiology. 2008;247:762–70. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical