Anesthesia and thyroid surgery: The never ending challenges
- PMID: 23776893
- PMCID: PMC3683195
- DOI: 10.4103/2230-8210.109671
Anesthesia and thyroid surgery: The never ending challenges
Abstract
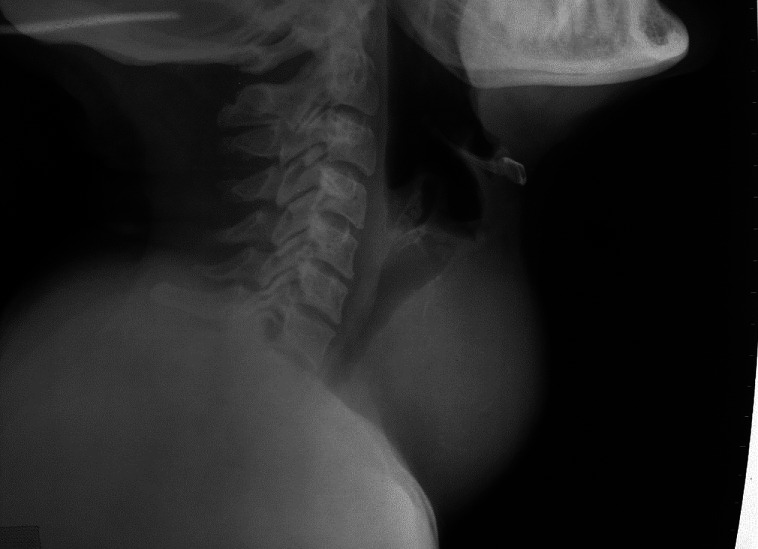
Thyroidectomy is the most common endocrine surgical procedure being carried out throughout the world. Besides, many patients who have deranged thyroid physiology, namely hyperthyroidism and hypothyroidism, have to undergo various elective and emergency surgical procedures at some stage of their life. The attending anesthesiologist has to face numerous daunting tasks while administering anesthesia to such patients. The challenging scenarios can be encountered at any stage, be it preoperative, intra-op or postoperative period. Preoperatively, deranged thyroid physiology warrants optimal preparation, while anticipated difficult airway due to enlarged thyroid gland further adds to the anesthetic challenges. Cardiac complications are equally challenging as also the presence of various co-morbidities which make the task of anesthesiologist extremely difficult. Thyroid storm can occur during intra-op and post-op period in inadequately prepared surgical patients. Postoperatively, numerous complications can develop that include hemorrhage, laryngeal edema, nerve palsies, tracheomalacia, hypocalcemic tetany, pneumothorax, etc., The present review aims at an in-depth analysis of potential risk factors and challenges during administration of anesthesia and possible complications in patients with thyroid disease.
Keywords: Airway management; carbimazole; propanolol; thyroid; thyroidectomy; thyroxin; tracheomalacia.
Conflict of interest statement
Figures


Similar articles
-
Anesthesia case management for thyroidectomy.AANA J. 2010 Apr;78(2):151-60. AANA J. 2010. PMID: 20583462 Review.
-
The thyroid gland.Contemp Anesth Pract. 1980;3:109-45. Contemp Anesth Pract. 1980. PMID: 7011668 Review.
-
Epilepsy and nonepilepsy surgery: Recent advancements in anesthesia management.Anesth Essays Res. 2013 Jan-Apr;7(1):10-7. doi: 10.4103/0259-1162.113978. Anesth Essays Res. 2013. PMID: 25885713 Free PMC article. Review.
-
Anesthetic management of primary hyperparathyroidism: A role rarely noticed and appreciated so far.Indian J Endocrinol Metab. 2013 Mar;17(2):235-9. doi: 10.4103/2230-8210.109679. Indian J Endocrinol Metab. 2013. PMID: 23776894 Free PMC article.
-
Advantages of recurrent laryngeal nerve identification in thyroidectomy and parathyroidectomy and the importance of preoperative and postoperative laryngoscopic examination in more than 1000 nerves at risk.Laryngoscope. 2002 Jan;112(1):124-33. doi: 10.1097/00005537-200201000-00022. Laryngoscope. 2002. PMID: 11802050
Cited by
-
Hypnosis in High-Intensity Focused Ultrasound for Thyroid Nodule Ablation.Am J Case Rep. 2023 Nov 19;24:e941524. doi: 10.12659/AJCR.941524. Am J Case Rep. 2023. PMID: 37980542 Free PMC article.
-
Endocrinopathies: The current and changing perspectives in anesthesia practice.Indian J Endocrinol Metab. 2015 Jul-Aug;19(4):462-9. doi: 10.4103/2230-8210.159026. Indian J Endocrinol Metab. 2015. PMID: 26180760 Free PMC article. Review.
-
Outcome Analysis of Total Thyroidectomy: Conventional Suture Ligation Technique vs Sutureless Technique.Cureus. 2023 Oct 30;15(10):e48005. doi: 10.7759/cureus.48005. eCollection 2023 Oct. Cureus. 2023. PMID: 38046490 Free PMC article.
-
Identifying predictors of a difficult thyroidectomy.J Surg Res. 2014 Jul;190(1):157-63. doi: 10.1016/j.jss.2014.03.034. Epub 2014 Mar 19. J Surg Res. 2014. PMID: 24750986 Free PMC article.
-
Post-operative analgesic efficacy of 0.25% ropivacaine with dexmedetomidine versus dexamethasone as an adjuvant in bilateral superficial cervical plexus block for thyroidectomy under general anaesthesia - A comparative randomized clinical study.Indian J Anaesth. 2023 Mar;67(3):269-276. doi: 10.4103/ija.ija_272_22. Epub 2023 Mar 16. Indian J Anaesth. 2023. PMID: 37250524 Free PMC article.
References
-
- Dionigi G, Dionigi R, Bartalena L, Tanda ML, Piantanida E, Castano P, et al. Current indications for thyroidectomy. Minerva Chir. 2007;62:359–72. - PubMed
-
- Agarwal G, Aggarwal V. Is total thyroidectomy the surgical procedure of choice for benign multinodular goiter? An evidence-based review. World J Surg. 2008;32:1313–24. - PubMed
-
- Farling PA. Thyroid disease. Br J Anesth. 2000;85:15–28. - PubMed
-
- White ML, Doherty GM, Gauger PG. Evidence-based surgical management of substernal goiter. World J Surg. 2008;32:1285–300. - PubMed
-
- Bouaggad A, Nejmi SE, Bouderka MA, Abbassi O. Prediction of difficult tracheal intubation in thyroid surgery. Anesth Analg. 2004;99:603–6. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous