

Cryoprecipitate use in the PROMMTT study
- PMID: 23778509
- PMCID: PMC3736696
- DOI: 10.1097/TA.0b013e31828fa3ed
Cryoprecipitate use in the PROMMTT study
Abstract
Background: There are few clinical data to guide the use of cryoprecipitate in severely injured trauma patients. Cryoprecipitate is a rich source of fibrinogen and has been associated with improved survival in animal as well as limited human studies. Our objectives were to identify patterns and predictors of cryoprecipitate use and determine whether transfusing cryoprecipitate was associated with improved survival.
Methods: This secondary analysis of 1,238 of 1,245 PRospective Observational Multicenter Major Trauma Transfusion (PROMMTT) study patients who had timed transfusion data included 359 (29%) who received cryoprecipitate. For this analysis, one dose of cryoprecipitate was defined as 10 U. Unadjusted predictors of cryoprecipitate use were identified using logistic regression. Multivariable time-dependent Cox models were performed to examine the association of cryoprecipitate on time to in-hospital death.
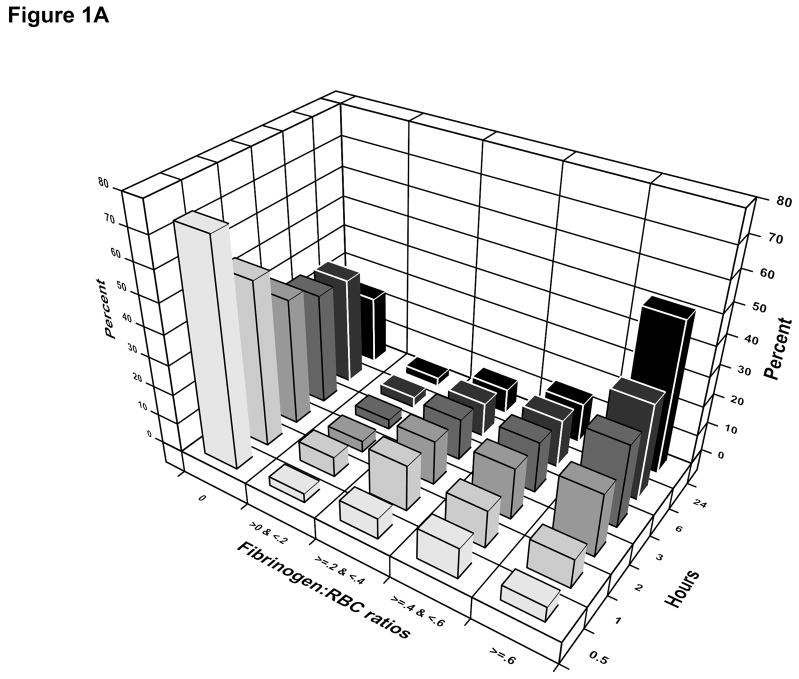
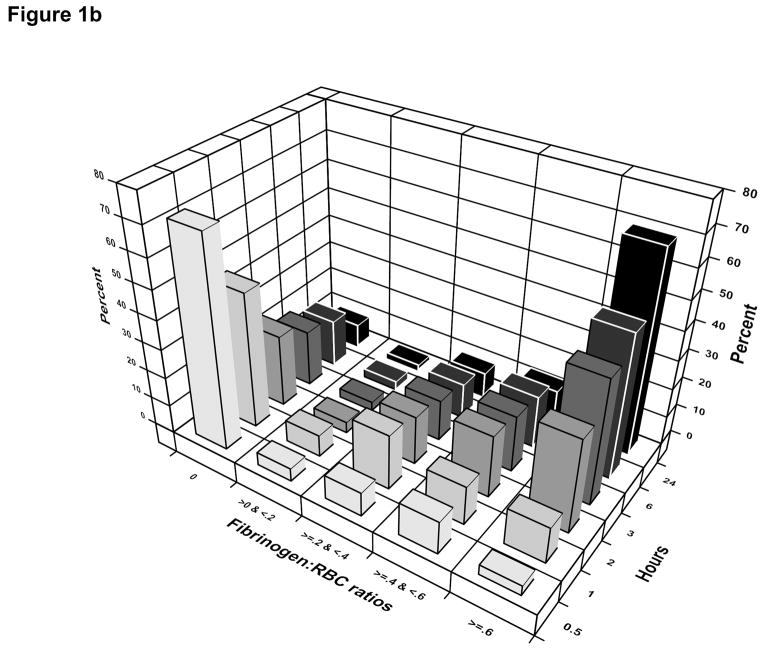
Results: Cryoprecipitate use varied significantly by center, ranging from 7% to 82%. Among patients who received cryoprecipitate, the median number of units infused by 24 hours was 10 (interquartile range, 10-20). The median time from admission to first cryoprecipitate unit was 2.7 hours (interquartile range, 1.7-4.4 hours). Of those who died of a hemorrhagic death within 6 hours of admission, 72% received no cryoprecipitate. Other unadjusted predictors of cryoprecipitate use included Injury Severity Score (ISS), initial fibrinogen levels, base deficit, international normalized ratio, prothrombin time/partial thromboplastin time, hemoglobin, damage-control surgery, and surgical intervention of the chest and abdomen. Cryoprecipitate use was not associated with in-hospital mortality after adjusting for initial pH, initial hemoglobin, emergency department systolic blood pressure, emergency department Glasgow Coma Scale (GCS) score, blood product use, ISS, and center.
Conclusion: Ten US Level 1 trauma centers vary greatly in their timing and use of cryoprecipitate in severely injured trauma patients. We could not identify any association of cryoprecipitate use with in-hospital mortality, although most patients did not receive this product. Randomized controlled studies are needed to determine if cryoprecipitate (or fibrinogen concentrates) have a beneficial effect.
Conflict of interest statement
Figures
References
-
- Evans JA, van Wessem KJ, McDougall D, Lee KA, Lyons T, Balogh ZJ. Epidemiology of traumatic deaths: comprehensive population-based assessment. World J Surg. 2010;34:158–163. - PubMed
-
- Borgman MA, Spinella PC, Perkins JG, Grathwohl KW, Repine T, Beekley AC, Sebesta J, Jenkins D, Wade CE, Holcomb JB. The ratio of blood products transfused affects mortality in patients receiving massive transfusions at a combat support hospital. J Trauma. 2007;63:805–813. - PubMed
-
- Holcomb JB, Jenkins D, Rhee P, Johannigman J, Mahoney P, Mehta S, Cox ED, Gehrke MJ, Beilman GJ, Schreiber M, et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007;62:307–310. - PubMed
-
- Holcomb JB, Wade CE, Michalek JE, Chisholm GB, Zarzabal LA, Schreiber MA, Gonzalez EA, Pomper GJ, Perkins JG, Spinella PC, et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann Surg. 2008;248:447–458. - PubMed
-
- Brohi K, Singh J, Heron M, Coats T. Acute traumatic coagulopathy. J Trauma. 2003;54:1127–1130. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
