

Clinical and mechanistic drivers of acute traumatic coagulopathy
- PMID: 23778510
- PMCID: PMC3755603
- DOI: 10.1097/TA.0b013e31828fa43d
Clinical and mechanistic drivers of acute traumatic coagulopathy
Abstract
Background: Acute traumatic coagulopathy (ATC) occurs after severe injury and shock and is associated with increased bleeding, morbidity, and mortality. The effects of ATC and hemostatic resuscitation on outcome are not well-explored. The PRospective Observational Multicenter Major Trauma Transfusion (PROMMTT) study provided a unique opportunity to characterize coagulation and the effects of resuscitation on ATC after severe trauma.
Methods: Blood samples were collected upon arrival on a subset of PROMMTT patients. Plasma clotting factor levels were prospectively assayed for coagulation factors. These data were analyzed with comprehensive PROMMTT clinical data.
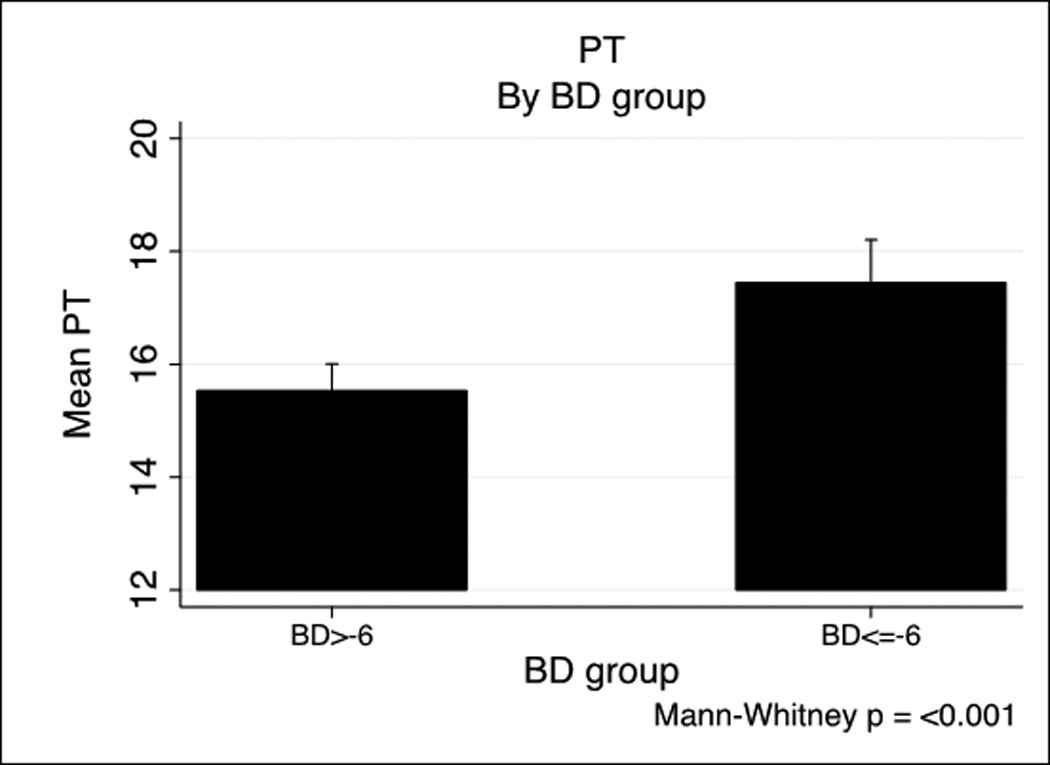
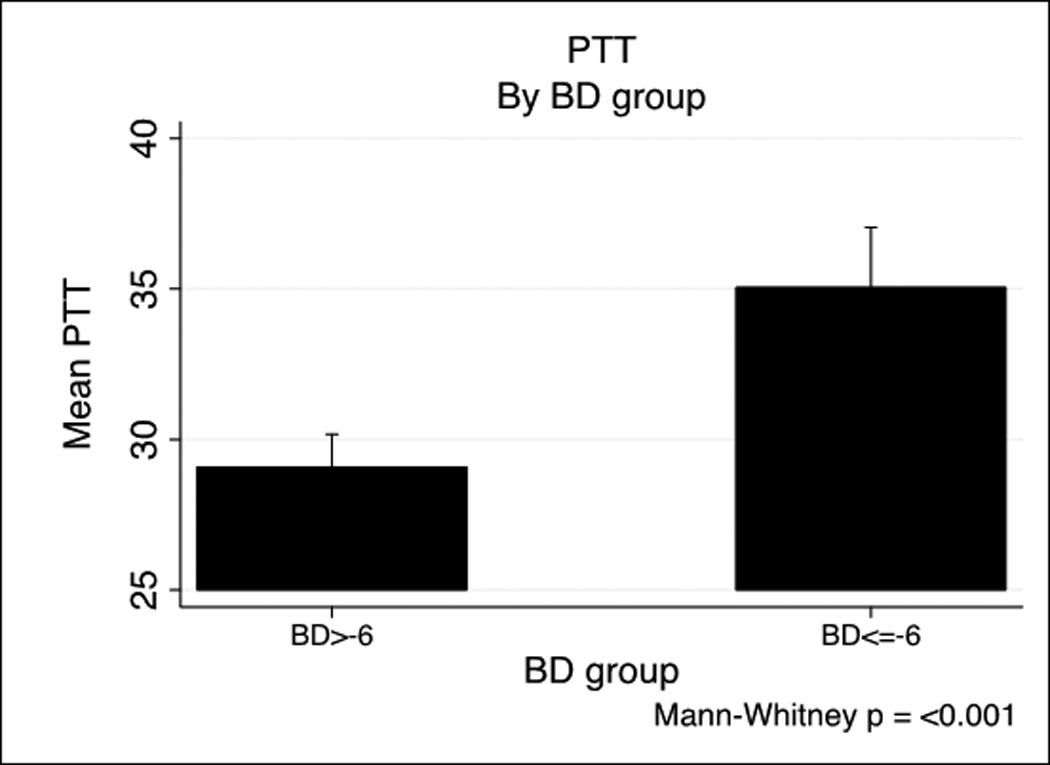
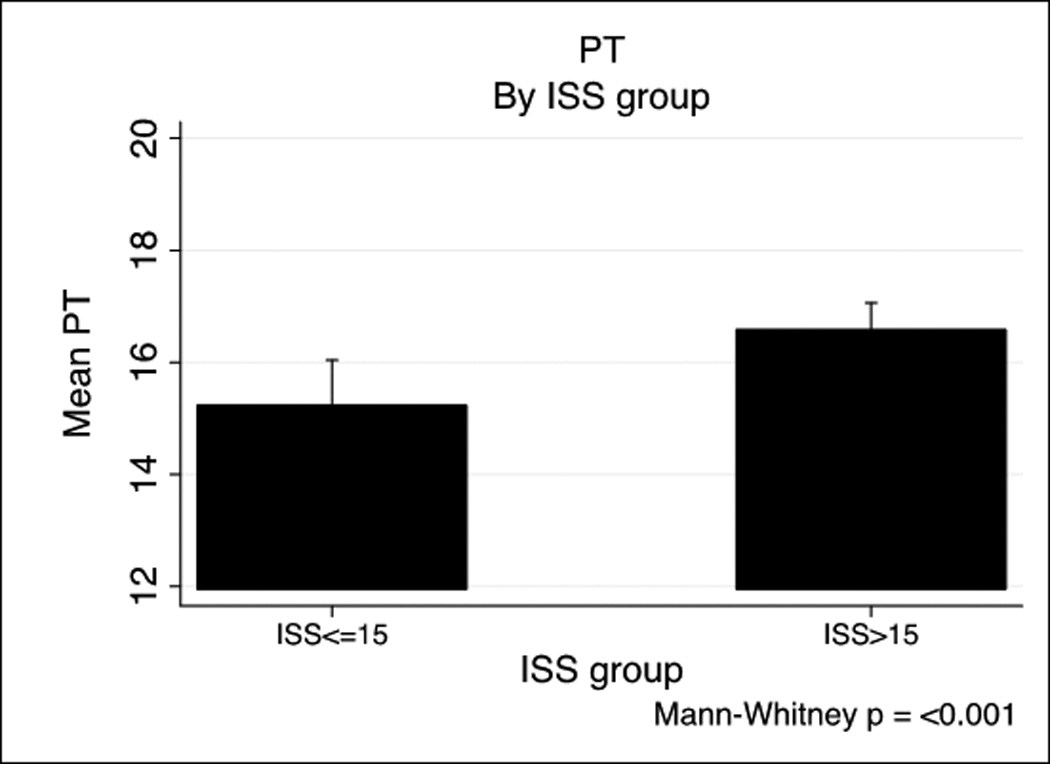
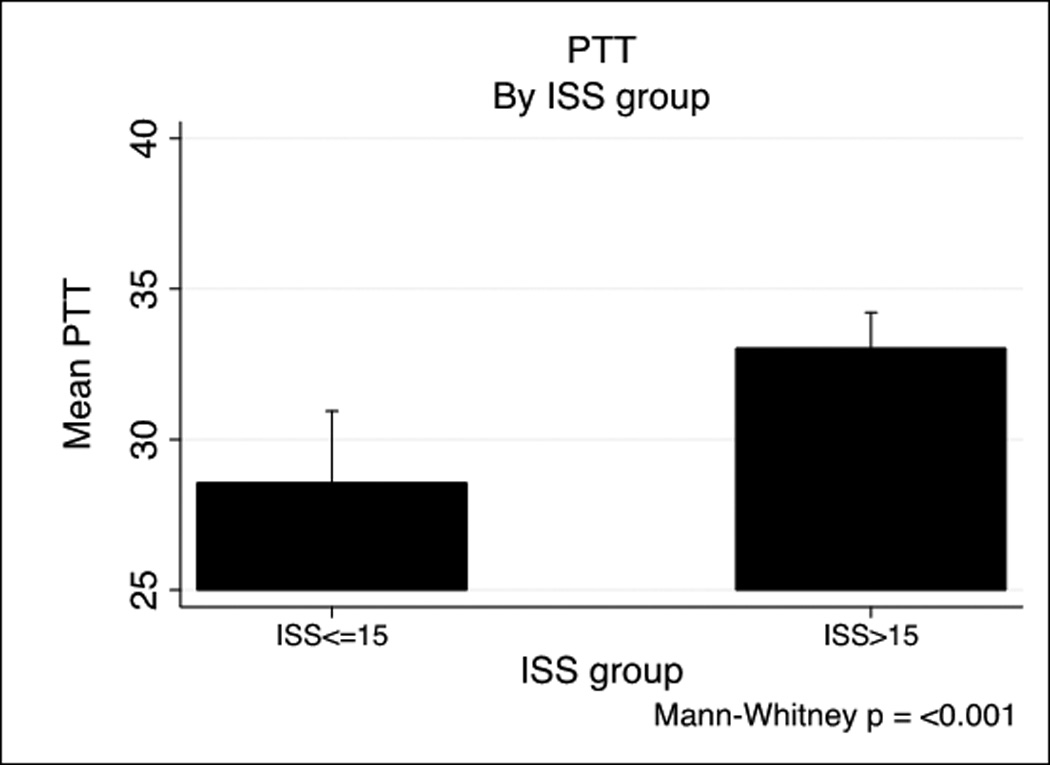
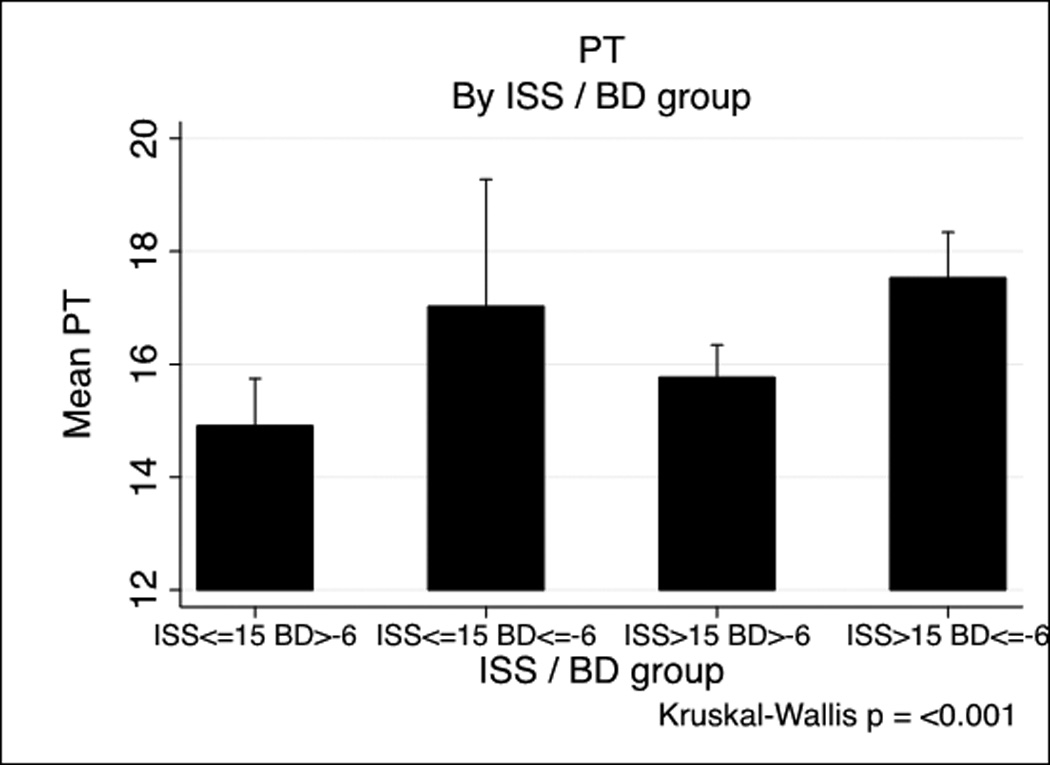
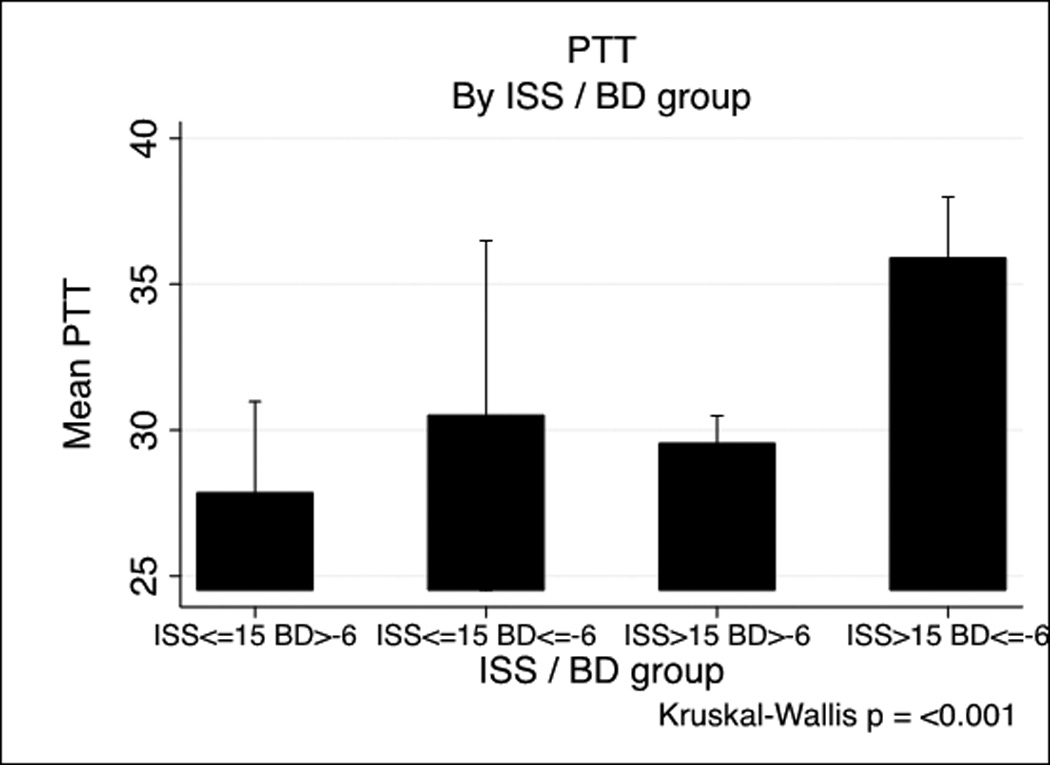
Results: There were 1,198 patients with laboratory results, of whom 41.6% were coagulopathic. Using international normalized ratio of 1.3 or greater, 41.6% of patients (448) were coagulopathic, while 20.5% (214) were coagulopathic using partial thromboplastin time of 35 or greater. Coagulopathy was primarily associated with a combination of an Injury Severity Score (ISS) of greater than 15 and a base deficit (BD) of less than -6 (p < 0.05). Regression modeling for international normalized ratio-based coagulopathy shows that prehospital crystalloid (odds ratio [OR], 1.05), ISS (OR, 1.03), Glasgow Coma Scale (GCS) score (OR, 0.93), heart rate (OR, 1.08), systolic blood pressure (OR, 0.96), BD (OR, 0.92), and temperature (OR, 0.84) were significant predictors of coagulopathy (all p < 0.03). A subset of 165 patients had blood samples collected and coagulation factor analysis performed. Elevated ISS and BD were associated with elevation of aPC and depletion of factors (all p < 0.05). Reductions in factors I, II, V, VIII and an increase in aPC drive ATC (all p < 0.04). Similar results were found for partial thromboplastin time-defined coagulopathy.
Conclusion: ATC is associated with the depletion of factors I, II, V, VII, VIII, IX, and X and is driven by the activation of the protein C system. These data provide additional mechanistic understanding of the drivers of coagulation abnormalities after injury. Further understanding of the drivers of ATC and the effects of resuscitation can guide factor-guided resuscitation and correction of coagulopathy after injury.
Conflict of interest statement
Figures
References
-
- Geneva: World Health Orginization; Injury Chart Book.
-
- Hess JR, Holcomb JB, Hoyt DB. Damage control resuscitation: the need for specific blood products to treat the coagulopathy of trauma. Transfusion. 2006;46(5):685–686. - PubMed
-
- Cohen MJ. Towards hemostatic resuscitation: the changing understanding of acute traumatic biology, massive bleeding, and damage-control resuscitation. The Surgical clinics of North America. 2012;92(4):877–891. - PubMed
-
- Howard BM, Daley AT, Cohen MJ. Prohemostatic interventions in trauma: resuscitation-associated coagulopathy, acute traumatic coagulopathy, hemostatic resuscitation, and other hemostatic interventions. Seminars in thrombosis and hemostasis. 2012;38(3):250–258. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
